Pronation of the foot
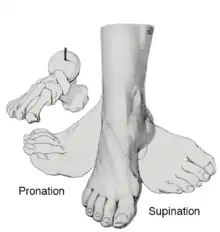
Pronation is a natural movement of the foot that occurs during foot landing while running or walking. Composed of three cardinal plane components: subtalar eversion, ankle dorsiflexion, and forefoot abduction,[1][2] these three distinct motions of the foot occur simultaneously during the pronation phase.[3] Pronation is a normal, desirable, and necessary component of the gait cycle.[4] Pronation is the first half of the stance phase, whereas supination starts the propulsive phase as the heel begins to lift off the ground.[5]
Types
The normal biomechanics of the foot absorb and direct the occurring throughout the gait whereas the foot is flexible (pronation) and rigid (supination) during different phases of the gait cycle. As the foot is loaded, eversion of the subtalar joint, dorsiflexion of the ankle, and abduction of the forefoot occur.[5][6] Pronation should not occur past the latter stages of midstance, as the normal foot should then supinate in preparation for toe-off.[7]
Abnormal pronation occurs when a foot pronates when it should supinate, or overpronates during a normal pronation period of the gait cycle. Approximately four degrees of pronation and supination are necessary to enable the foot to propel forward properly. In the neutral position, the foot is neither pronating nor supinating. If the foot is pronating or supinating during the stance phase of the gait cycle when it ought to be in the neutral position, a biomechanical problem may exist.[3]
For ease of choosing corrective footwear, three types of pronation are recognized: neutral pronation, overpronation, and underpronation.[8]
Neutral pronation
Some pronation, also called eversion, is natural in the body’s regular movement. Neutral pronation occurs when the foot experiences a normal, healthy amount of pronation instead of overpronating or underpronating. In healthy movement, more of the toe area will be used when pushing off than an unhealthy movement.[9] In neutral pronation, the weight distributes fairly evenly among all of the toes with a slight emphasis on the big toe and second toe, which are better adapted to handle more of the load.[8]
Overpronation

Those who overpronate tend to push off almost completely from the big toe and second toe. As a result, the shock from the foot’s impact doesn’t spread evenly throughout the foot and the ankle has trouble stabilizing the rest of the body. Additionally, an unnatural angle forms between the foot and ankle and the foot splays out abnormally. It is common even for people who pronate normally to have some angle between the foot and the ankle, but not to the extent seen in those who overpronate. In normal pronation, the weight distributes evenly throughout the foot.[8]
Causes
There are many possible causes for overpronation, but researchers have not yet determined an underlying cause. Hintermann states, “Compensatory overpronation may occur for anatomical reasons, such as a tibia vara of 10 degrees or more, forefoot varus, leg length discrepancy, ligamentous laxity, or because of muscular weakness or tightness in the gastrocnemius and soleus muscles."[9] Pronation can be influenced by sources outside of the body as well. Shoes have been shown to significantly influence pronation. Hintermann states that the same person can have different amounts of pronation just by using different running shoes. “It is easily possible that the maximal ankle joint eversion movement is 31 degrees for one and 12 degrees for another running shoe."[9]

There has been some speculation as to whether arch height has an effect on pronation. After conducting a study at the Rose-Hulman Institute of Technology, Maggie Boozer suggests that people with higher arches tend to pronate to a greater degree.[10] However, the generally accepted view by professionals is that the most pronation is present in those with lower arch heights.[8] To complicate matters, one study done by Hylton Menz at the University of Western Sydney-Macarthur suggests that the methods for measuring arch height and determining whether someone is “flat-footed” or “high-arched” are unreliable. He says, “For this reason, studies investigating the relationship between static arch height motion of the rearfoot have consistently found that such a classification system is a poor predictor of dynamic rearfoot function.”[11]
Effects
Overpronation may have secondary effects on the lower legs, such as increased rotation of the tibia, which may result in lower leg or knee problems. Overpronation is usually associated with many overuse injuries in running including medial tibial stress syndrome,[12] or shin splints, and knee pain[9] Hintermann states, “Individuals with injuries typically have pronation movement that is about two to four degrees greater than that of those with no injuries.” He adds however, that between 40% and 50% of runners who overpronate do not have overuse injuries. This suggests that although pronation may have an effect on certain injuries, it is not the only factor influencing their development.
Orthotics
The design principles of foot orthoses are founded on knowledge of the functional anatomy of the foot. Pronation of the foot is triplanar. The axis of rotation in the foot joints is not perpendicular to any of the cardinal planes (sagittal, horizontal, frontal) of the human body. The triplanar motion of the foot postulates that blocking of any one component of triplanar motion in a single cardinal plane prevents movement in the other two planes as well. This all-or-nothing rule is the premise for orthotic posting or wedging.[13]
Supportive orthotics in the shoe is a method commonly implemented to treat many common running injuries associated with excessive pronation. Orthotics are the most effective treatment for symptoms that develop from biomechanics within the body such as overpronation, resulting in either great improvement or complete healing of the injury in about half the cases.[14]
Shoe type
Foot pronation tends to increase in runners as mileage also increases, potentially increasing the risk for injury.[15] Motion control shoes are a specific type of running shoe designed to limit these excessive foot motions by reducing the amount of plantar force (a force generated by excess pronation). Motion control and stability shoes have increased medial support which may increase stability to the foot and leg and lower the amount of pronation in the foot.[9]
Taping
Certain methods of taping the foot and leg have also been shown to be effective in preventing overpronation. In a study conducted at the University of Queensland, a taping procedure known as the LowDye taping technique was shown to be effective in controlling pronation during both movement and standing.[16]
Shoe-lacing patterns
Specific patterns of lacing running shoes also reduce pronation. Pronation significantly decreases when the highest number of eyelets in the shoe is used for lacing and the shoes are tied as tight as possible,[17]

Barefoot running
Several studies have shown that running barefoot can decrease pronation on the foot’s impact with the ground. This is thought to be because running shoes have extra weight for cushioning at the heel of the shoe, causing the runner to heel-strike more, which in turn results in increased pronation during the step. According to researchers at the Biomechanics Laboratory of the Swiss Federal Institute of Technology, “The least amount of pronation takes place when running barefoot."[18]
Supination
Supination is the opposite, and occurs when the foot impacts the ground and there is not enough of an “inward roll” in the foot’s motion. The weight of the body isn’t transferred at all to the big toe, forcing the outside of the foot and the smaller toes which can't handle the stress as well to take the majority of the overweight instead.
Runner’s World states, “[Underpronators] do best in a neutral-cushioned shoe that encourages a more natural foot motion."[8] Since underpronators’ feet don’t roll inward like overpronators’, support isn’t necessarily needed to correct supination as it is to correct overpronation.
References
- Joseph E. Muscolino (14 April 2014). Kinesiology: The Skeletal System and Muscle Function. Elsevier Health Sciences. pp. 315–. ISBN 978-0-323-29142-2.
- David J. Magee (25 March 2014). Orthopedic Physical Assessment. Elsevier Health Sciences. pp. 915–. ISBN 978-1-4557-0975-5.
- Glenn Copeland; Stan Solomon; Mark Myerson (2004). The Good Foot Book: A Guide for Men, Women, Children, Athletes, Seniors--everyone. Hunter House. pp. 19–. ISBN 978-0-89793-448-0.
- Jeffrey Bytomski; Claude Moorman (2 April 2010). Oxford American Handbook of Sports Medicine. Oxford University Press. pp. 342–. ISBN 978-0-19-970717-1.
- Jonathan T. Finnoff, DO; Mark A. Harrast, MD (18 November 2011). Sports Medicine: Study Guide and Review for Boards. Demos Medical Publishing. pp. 37–. ISBN 978-1-61705-054-1.
- William J. Koopman; Dennis W. Boulware; Gustavo R. Heudebert (2003). Clinical Primer of Rheumatology. Lippincott Williams & Wilkins. pp. 49–. ISBN 978-0-683-30648-4.
- Domhnall MacAuley (1 November 2012). Oxford Handbook of Sport and Exercise Medicine. OUP Oxford. pp. 692–. ISBN 978-0-19-101593-9.
- "Pronation, Explained". Runner's World. February 23, 2005.
- Hintermann B, Nigg BM (September 1998). "Pronation in runners. Implications for injuries". Sports Med. 26 (3): 169–76. doi:10.2165/00007256-199826030-00003. PMID 9802173.
- Boozer MH, Finch A, Waite LR (2002). "Investigation of the relationship between arch height and maximum pronation angle during running". Biomed Sci Instrum. 38: 203–7. PMID 12085602.
- Menz HB (March 1998). "Alternative techniques for the clinical assessment of foot pronation". J Am Podiatr Med Assoc. 88 (3): 119–29. doi:10.7547/87507315-88-3-119. PMID 9542353.
- Tweed JL, Campbell JA, Avil SJ (2008). "Biomechanical risk factors in the development of medial tibial stress syndrome in distance runners". J Am Podiatr Med Assoc. 98 (6): 436–44. doi:10.7547/0980436. PMID 19017851.
- Michelle M. Lusardi; Millee Jorge; Caroline C. Nielsen (23 December 2013). Orthotics and Prosthetics in Rehabilitation. Elsevier Health Sciences. pp. 193–. ISBN 978-0-323-29134-7.
- Gross ML, Davlin LB, Evanski PM (1991). "Effectiveness of orthotic shoe inserts in the long-distance runner". Am J Sports Med. 19 (4): 409–12. doi:10.1177/036354659101900416. PMID 1897659.
- Cheung RT, Ng GY (May 2008). "Influence of different footwear on force of landing during running". Phys Ther. 88 (5): 620–8. doi:10.2522/ptj.20060323. PMID 18276937.
- Vicenzino B, Franettovich M, McPoil T, Russell T, Skardoon G (December 2005). "Initial effects of anti-pronation tape on the medial longitudinal arch during walking and running". Br J Sports Med. 39 (12): 939–43, discussion 943. doi:10.1136/bjsm.2005.019158. PMC 1725092. PMID 16306503.
- Hagen M, Hennig EM (February 2009). "Effects of different shoe-lacing patterns on the biomechanics of running shoes". J Sports Sci. 27 (3): 267–75. doi:10.1080/02640410802482425. PMID 19156560.
- Stacoff A, Kälin X, Stüssi E (April 1991). "The effects of shoes on the torsion and rearfoot motion in running". Med Sci Sports Exerc. 23 (4): 482–90. doi:10.1249/00005768-199104000-00015. PMID 1676133.