Cardiac marker
Cardiac markers are biomarkers measured to evaluate heart function. They can be useful in the early prediction or diagnosis of disease.[1] Although they are often discussed in the context of myocardial infarction, other conditions can lead to an elevation in cardiac marker level.
| Cardiac marker | |
|---|---|
| LOINC | 58260-1 |
Most of the early markers identified were enzymes, and as a result, the term "cardiac enzymes" is sometimes used. However, not all of the markers currently used are enzymes. For example, in formal usage, troponin would not be listed as a cardiac enzyme.[2]
Applications of measurement
Measuring cardiac biomarkers can be a step toward making a diagnosis for a condition. Whereas cardiac imaging often confirms a diagnosis, simpler and less expensive cardiac biomarker measurements can advise a physician whether more complicated or invasive procedures are warranted. In many cases medical societies advise doctors to make biomarker measurements an initial testing strategy especially for patients at low risk of cardiac death.[3][4]
Many acute cardiac marker IVD products are targeted at nontraditional markets, e.g., the hospital ER instead of traditional hospital or clinical laboratory environments. Competition in the development of cardiac marker diagnostic products and their expansion into new markets is intense.[5]
Recently, the intentional destruction of myocardium by alcohol septal ablation has led to the identification of additional potential markers.[6]
Types
Types of cardiac markers include the following:
| Test | Sensitivity and specificity | Approximate peak | Description |
|---|---|---|---|
| Troponin test | The most sensitive and specific test for myocardial damage. Because it has increased specificity compared with CK-MB, troponin is composed of 3 proteins- Troponin C, Cardic troponin I, and Cardiac troponin T. Troponin I especially has a high affinity for myocardial injury. | 12 hours | Troponin is released during MI from the cytosolic pool of the myocytes. Its subsequent release is prolonged with degradation of actin and myosin filaments. Isoforms of the protein, T and I, are specific to myocardium. Differential diagnosis of troponin elevation includes acute infarction, severe pulmonary embolism causing acute right heart overload, heart failure, myocarditis. Troponins can also calculate infarct size but the peak must be measured in the 3rd day. After myocyte injury, troponin is released in 2–4 hours and persists for up to 7 days. Normal value are- Troponin I <0.3 ng/ml and Troponin T <0.2 ng/ml |
| Creatine Kinase (CK-MB) test | It is relatively specific when skeletal muscle damage is not present. | 10–24 hours | The CK-MB isoform of creatine kinase is expressed in heart muscle. It resides in the cytosol and facilitates movement of high energy phosphates into and out of mitochondria. Since it has a short duration, it cannot be used for late diagnosis of acute MI but can be used to suggest infarct extension if levels rise again. This is usually back to normal within 2–3 days. Normal range- 2-6 ng/ml |
| Lactate dehydrogenase (LDH) | LDH is not as specific as troponin. | 72 hours | Lactate dehydrogenase catalyses the conversion of pyruvate to lactate. LDH-1 isozyme is normally found in the heart muscle and LDH-2 is found predominantly in blood serum. A high LDH-1 level to LDH-2 suggest MI. LDH levels are also high in tissue breakdown or hemolysis. It can mean cancer, meningitis, encephalitis, or HIV. This is usually back to normal 10–14 days. |
| Aspartate transaminase (AST) | This was the first used.[7] It is not specific for heart damage, and it is also one of the liver transaminases. | ||
| Myoglobin (Mb) | low specificity for myocardial infarction | 2 hours | Myoglobin is used less than the other markers. Myoglobin is the primary oxygen-carrying pigment of muscle tissue. It is high when muscle tissue is damaged but it lacks specificity. It has the advantage of responding very rapidly,[8] rising and falling earlier than CK-MB or troponin. It also has been used in assessing reperfusion after thrombolysis.[9] |
| Ischemia-modified albumin (IMA) | low specificity | IMA can be detected via the albumin cobalt binding (ACB) test, a limited available FDA approved assay. Myocardial ischemia alters the N-terminus of albumin reducing the ability of cobalt to bind to albumin. IMA measures ischemia in the blood vessels and thus returns results in minutes rather than traditional markers of necrosis that take hours. ACB test has low specificity therefore generating high number of false positives and must be used in conjunction with typical acute approaches such as ECG and physical exam. Additional studies are required. | |
| Pro-brain natriuretic peptide | This is increased in patients with heart failure. It has been approved as a marker for acute congestive heart failure. Pt with < 80 have a much higher rate of symptom-free survival within a year. Generally, pt with CHF will have > 100. | ||
| Glycogen phosphorylase isoenzyme BB | 0.854 and 0.767[10] | 7 hours |
Glycogen phosphorylase isoenzyme BB (abbreviation: GPBB) is one of the three isoforms of glycogen phosphorylase. This isoform of the enzyme exists in cardiac (heart) and brain tissue. Because of the blood–brain barrier, GP-BB can be seen as being specific to heart muscle. GP-BB is one of the "new cardiac markers" which are considered to improve early diagnosis in acute coronary syndrome. During the process of ischemia, GP-BB is converted into a soluble form and is released into the blood. A rapid rise in blood levels can be seen in myocardial infarction and unstable angina. GP-BB is elevated 1–3 hours after process of ischemia. |
Limitations
Depending on the marker, it can take between 2 and 24 hours for the level to increase in the blood. Additionally, determining the levels of cardiac markers in the laboratory - like many other lab measurements - takes substantial time. Cardiac markers are therefore not useful in diagnosing a myocardial infarction in the acute phase. The clinical presentation and results from an ECG are more appropriate in the acute situation.
However, in 2010, research at the Baylor College of Medicine revealed that, using diagnostic nanochips and a swab of the cheek, cardiac biomarker readings from saliva can, with the ECG readings, determine within minutes whether someone is likely to have had a heart attack.
- Comparison of cardiac markers over time
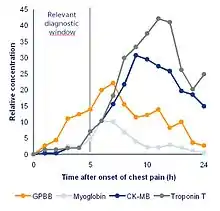 Comparison of cardiac marker in the first hours after chestpain onset and the relative concentration.
Comparison of cardiac marker in the first hours after chestpain onset and the relative concentration. Comparison of cardiac marker in the first hours after chestpain onset and the multiples of the cutoff.
Comparison of cardiac marker in the first hours after chestpain onset and the multiples of the cutoff.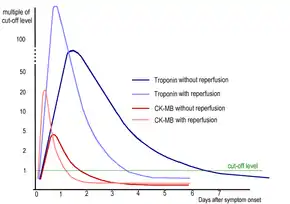 Kinetics of cardiac markers in myocardial infarction with or without reperfusion treatment.
Kinetics of cardiac markers in myocardial infarction with or without reperfusion treatment.
See also
- Myocardial markers in myocardial infarction
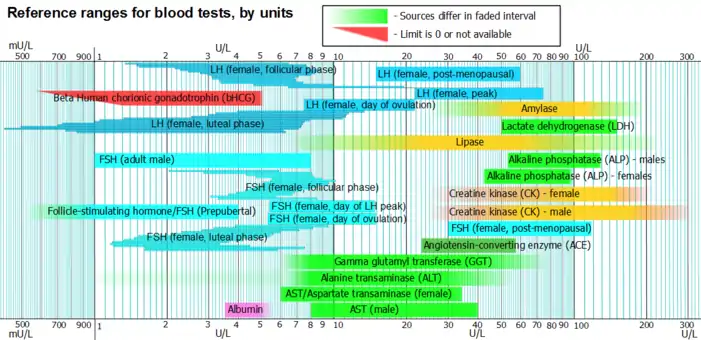
- Reference ranges for blood tests#Cardiac tests
References
- Rao SP, Miller S, Rosenbaum R, Lakier JB (2019). "Opportunities for microRNAs in the Crowded Field of Cardiovascular Biomarkers". Annual Review of Pathology: Mechanisms of Disease. 14: 211–238. doi:10.1146/annurev-pathmechdis-012418-012827. PMC 6442682. PMID 30332561.
- Rao SP, Miller S, Rosenbaum R, Lakier JB (August 1999). "Cardiac troponin I and cardiac enzymes after electrophysiologic studies, ablations, and defibrillator implantations". Am. J. Cardiol. 84 (4): 470, A9. doi:10.1016/S0002-9149(99)00337-9. PMID 10468091.
- American Society of Nuclear Cardiology, "Five Things Physicians and Patients Should Question" (PDF), Choosing Wisely: an initiative of the ABIM Foundation, American Society of Nuclear Cardiology, archived from the original (PDF) on 2012-04-16, retrieved August 17, 2012
- Hendel, R. C.; Berman, D. S.; Di Carli, M. F.; Heidenreich, P. A.; Henkin, R. E.; Pellikka, P. A.; Pohost, G. M.; Williams, K. A.; American College of Cardiology Foundation Appropriate Use Criteria Task Force; American Society of Nuclear Cardiology; American College Of, R.; American Heart, A.; American Society of Echocardiology; Society of Cardiovascular Computed Tomography; Society for Cardiovascular Magnetic Resonance; Society Of Nuclear, M. (2009). "ACCF/ASNC/ACR/AHA/ASE/SCCT/SCMR/SNM 2009 Appropriate Use Criteria for Cardiac Radionuclide Imaging". Journal of the American College of Cardiology. 53 (23): 2201–2229. doi:10.1016/j.jacc.2009.02.013. PMID 19497454.
- "Cardiac Marker Diagnostic Testing Markets". TriMark Publications, LLC. November 2011.
- Lewis GD; Wei R; Liu E; et al. (October 2008). "Metabolite profiling of blood from individuals undergoing planned myocardial infarction reveals early markers of myocardial injury". J. Clin. Invest. 118 (10): 3503–12. doi:10.1172/JCI35111. PMC 2525696. PMID 18769631.
- NISSEN NI, RANLOV P, WEIS-FOGH J (July 1965). "EVALUATION OF FOUR DIFFERENT SERUM ENZYMES IN THE DIAGNOSIS OF ACUTE MYOCARDIAL INFARCTION". Br Heart J. 27 (4): 520–6. doi:10.1136/hrt.27.4.520. PMC 503341. PMID 14324110.
- "Use of Cardiac Markers in the Emergency Department: - eMedicine". Retrieved 2009-01-06.
- Christenson RH; Ohman EM; Topol EJ; et al. (September 1997). "Assessment of coronary reperfusion after thrombolysis with a model combining myoglobin, creatine kinase-MB, and clinical variables. TAMI-7 Study Group. Thrombolysis and Angioplasty in Myocardial Infarction-7". Circulation. 96 (6): 1776–82. doi:10.1161/01.cir.96.6.1776. PMID 9323061.
- Lippi, G.; Mattiuzzi, C.; Comelli, I.; Cervellin, G. (2013). "Glycogen phosphorylase isoenzyme BB in the diagnosis of acute myocardial infarction: a meta-analysis". Biochem Med (Zagreb). 23 (1): 78–82. doi:10.11613/bm.2013.010. PMC 3900091. PMID 23457768.
Further reading
- Ross G, Bever F, Uddin Z, Devireddy L, Gardin J (2004). "Common scenarios to clarify the interpretation of cardiac markers". J Am Osteopath Assoc. 104 (4): 165–76. PMID 15127984.Full text
on GPBB