Cryoneurolysis
Cryoneurolysis, also referred to as cryoanalgesia, is a medical procedure that temporarily blocks nerve conduction along peripheral nerve pathways. The procedure, which inserts a small probe to freeze the target nerve, can facilitate complete regeneration of the structure and function of the affected nerve. Cryoneurolysis has been used to treat a variety of painful conditions.
| Cryoneurolysis | |
|---|---|
| Specialty | neurology |
Medical uses
A similar procedure that uses radiofrequency energy for back pain appears to have short term benefit, but it is unclear if it has a long term effect.[1]
Mechanisms of action
Nerve anatomy
Each nerve is composed of a bundle of axons. Each axon is surrounded by the endoneurium connective tissue layer. These axons are bundled into fascicles surrounded by the perineurium connective tissue layer. Multiple fascicles are then surrounded by the epineurium, which is the outermost connective tissue layer of the nerve. The axons of myelinated nerves have a myelin sheath made up of Schwann cells that coat the axon.[2]
Nerve injury classification
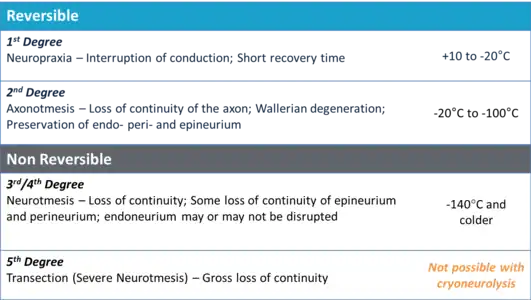
Classification of nerve damage was well-defined by Sir Herbert Seddon and Sunderland in a system that remains in use.[6] The adjacent table details the forms (neurapraxia, axonotmesis and neurotmesis) and degrees of nerve injury that occur as a result of exposure to various temperatures.
Cryoneurolysis treatments that use nitrous oxide (boiling point of -88.5 °C) as the coolant fall in the range of an axonotmesis injury, or 2nd degree injury, according to the Sunderland classification system. Treatments of the nerve in this temperature range are reversible. Nerves treated in this temperature range experience a disruption of the axon, with Wallerian degeneration occurring distal to the site of injury.[7] The axon and myelin sheath are affected, but all of the connective tissues (endoneurium, perineurium, and epineurium) remain intact.[8] Following Wallerian degeneration, the axon regenerates along the original nerve path at a rate of approximately 1–2 mm per day.[9][10][11][12]
Cryoneurolysis differs from cryoablation in that cryoablation treatments utilize liquid nitrogen (boiling point of -195.8 °C) as the coolant, and therefore, fall into the range of a neurotmesis injury, or 3rd degree injury according to the Sunderland classification. Treatments of the nerve in this temperature range are irreversible. Nerves treated in this temperature range experience a disruption of both the axon and the endoneurium connective tissue layer.[13][14]
History
The use of cold for pain relief and as an anti-inflammatory has been known since the time of Hippocrates (460-377 B.C).[15] Since then there have been numerous accounts of ice used for pain relief including from the Ancient Egyptians and Avicenna of Persia (A.D.982–1070).[16] In 1812 Napoleon's Surgeon General noted that half-frozen soldiers from the Moscow battle were able to tolerate amputations with reduced pain[17] and in 1851, ice and salt mixtures were promoted by Arnott for the treatment of nerve pain. Campbell White, in 1899, was the first to use refrigerants medically, and Allington, in 1950, was the first to use liquid nitrogen for medical treatments.[15] In 1961, Cooper et al. created an early cryoprobe that reached -190 °C using liquid nitrogen.[15] Shortly thereafter, in 1967, an ophthalmic surgeon named Amoils used carbon dioxide and nitrous oxide to create a cryoprobe that reached -70 °C.[15]
Devices
Cryoprobe
Cryoneurolysis is performed with a cryoprobe, which is composed of a hollow cannula that contains a smaller inner lumen. The pressurized coolant (nitrous oxide, carbon dioxide or liquid nitrogen) travels down the lumen and expands at the end of the lumen into the tip of the hollow cannula. No coolant exits the cryoprobe. The expansion of the pressurized liquid causes the surrounding area to cool (known as the Joule-Thomson effect) and the phase change of the liquid to gas also causes the surrounding area to cool. This causes a visible iceball to form and the tissue surrounding the end of the cryoprobe to freeze. The gas form of the coolant then travels up the length of the cryoprobe and is safely expelled. The tissue surrounding the end of the cryoprobe can reach as low as -88.5 °C with nitrous oxide as the coolant, and as low as -195.8 °C with liquid nitrogen. Temperatures below -100 °C are damaging to nerves.

CRYO-S PAINLESS Cryoanalgesia device is the next generation of apparatus used by many experts in the field since 1992. The working medium for CRYO-S PAINLESS is carbon dioxide: CO2 (-78°C) or nitrous oxide: N2O (-89°C), very efficient and easy to use gases.CRYO-S PAINLESS is controlled by a microprocessor and all the parameters are displayed and monitored on a LCD screen. Mode selection probe, cleaning and freezing can be performed automatically using footswitch or touch screen which allows to keep the site of a procedure under sterile conditions. Electronic communication (chip system) between the connected probe and device allows recognition of optimal operating parameters and auto-configures to cryoprobe characteristics. Pressure and gas flow are set automatically, any manual adjustment is not necessary. Cryoprobe temperature, cylinder pressure, gas flow inside of cryoprobe and procedure time are displayed during freezing. Built-in voice communication Built-in neurostimulation (sensory, motor).
Other Devices
The Endocare PerCryo Percutaneous Cryoablation device utilizes argon as a coolant and can be used with 4 different single cryoprobe configurations with a diameter of either 1.7 mm (~16 gauge) or 2.4 mm (~13 gauge) in diameter .[18]
The Myoscience Iovera° is a handheld device that uses nitrous oxide as a coolant and can be used with a three-probe configuration with a probe diameter of 0.4 mm (~27 gauge).[19]
References
- Boswell, MV; Colson, JD; Sehgal, N; Dunbar, EE; Epter, R (January 2007). "A systematic review of therapeutic facet joint interventions in chronic spinal pain". Pain Physician. 10 (1): 229–53. PMID 17256032.
- Gray, Henry (1918). Gray's Anatomy. Philadelphia: Lea & Febiger. ISBN 1-58734-102-6.
- Zhou, L; Kambin, P; Casey, KF; Bonner, FJ; O'Brien, E; Shao, Z; Ou, S (August 1995). "Mechanism research of cryoanalgesia". Neurological Research. 17 (4): 307–311. doi:10.1080/01616412.1995.11740333. PMID 7477749.
- Sunderland (1968). Nerves and Nerve Injuries. Edinburgh & London: Livingstone. p. 180.
- Zhou (2003). "Cryoanalgesia: electrophysiology at different temperatures". Cryobiology. 46 (1): 26–32. doi:10.1016/s0011-2240(02)00160-8. PMID 12623025.
- Seddon HJ (1943). "Three Types of Nerve Injury". Brain. 66 (4): 238–288. doi:10.1093/brain/66.4.237.
- Savastano (2014). "Sciatic nerve injury: A simple and subtle model for investigating many aspects of nervous system damage and recovery". Journal of Neuroscience Methods. 227: 166–180. doi:10.1016/j.jneumeth.2014.01.020.
- Hsu (2013). "Reduction in muscular motility by selective focused cold therapy". Journal of Neural Transmission. 121 (1): 15–20. doi:10.1007/s00702-013-1077-y. PMC 3889817. PMID 23917804.
- Evans (1981). "Cryoanalgesia: the response to alterations in freeze cycle and temperature". British Journal of Anaesthesia. 53 (11): 1121–1127. doi:10.1093/bja/53.11.1121. PMID 7326160.
- Tetzlaff (1989). "Neurofilament elongation into regenerating facial nerve axons". Neuroscience. 29 (3): 659–666. doi:10.1016/0306-4522(89)90138-3. PMID 2500618.
- Seil (1983). Nerve, organ, and tissue regeneration--research perspectives (xv ed.). New York: Academic Press. p. 482.
- Lundy-Eckman (2007). Neuroscience: Fundamentals for rehabilitation (3rd ed.). St. Louis, MIssouri: Elsevier Saunders.
- Sunderland (1951). "A classification of peripheral nerve injuries producing loss of function". Brain. 74 (4): 491–516. doi:10.1093/brain/74.4.491. PMID 14895767.
- Burnett (2004). "Pathophysiology of peripheral nerve injury: a brief review". Neurosurgical Focus. 16 (5): E1. doi:10.3171/foc.2004.16.5.2. PMID 15174821.
- Cooper (2001). "The History of Cryosurgery". Journal of the Royal Society of Medicine. 94 (4): 196–201. doi:10.1177/014107680109400416. PMC 1281398. PMID 11317629.
- Trescott (2003). "Cryoanalgesia in Interventional Pain Management". Pain Physician. 6: 345–360.
- Larrey, Dominique Jean (1832). Surgical Memoirs of the campaigns of Russia, Germany and France. Philadelphia: Carey & Lea.
- "The perfect Percryo probe for any procedure" (PDF). HealthTronics. Retrieved April 11, 2015.
- "Iovera Health - How it Works". Myoscience. Archived from the original on April 12, 2015. Retrieved April 11, 2015.