Streptococcus agalactiae
Streptococcus agalactiae (also known as group B streptococcus or GBS) is a gram-positive coccus (round bacterium) with a tendency to form chains (as reflected by the genus name Streptococcus). It is a beta-hemolytic, catalase-negative, and facultative anaerobe.[1][2]
| Streptococcus agalactiae | |
|---|---|
| Scientific classification | |
| Domain: | |
| Phylum: | |
| Class: | |
| Order: | |
| Family: | |
| Genus: | |
| Species: | S. agalactiae |
| Binomial name | |
| Streptococcus agalactiae Lehmann and Neumann, 1896 | |
S. agalactiae is the species designation for the only species of streptococci belonging to the group B of the Rebecca Lancefield classification of streptococci. GBS is surrounded by a bacterial capsule composed of polysaccharides (exopolysacharide). The species is subclassified into ten serotypes (Ia, Ib, II–IX) depending on the immunologic reactivity of their polysaccharide capsule.[1][3][4] This is why the plural term group B streptococci (referring to the serotypes) and the singular term group B streptococcus (referring to the single species) are both commonly encountered.
In general, GBS is a harmless commensal bacterium being part of the human microbiota colonizing the gastrointestinal and genitourinary tract of up to 30% of healthy human adults (asymptomatic carriers). Nevertheless, GBS can cause severe invasive infections especially in newborns, the elderly, and people with compromised immune systems.[5]

S. agalactiae is also a common veterinary pathogen, because it can cause bovine mastitis (inflammation of the udder) in dairy cows. The species name agalactiae meaning "of no milk", alludes to this.[6]

Laboratory identification
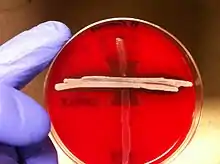
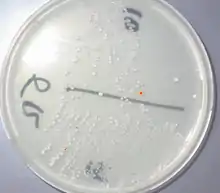
GBS grows readily on blood agar plates as colonies surrounded by a narrow zone of β-hemolysis. GBS is characterized by the presence in the cell wall of the antigen group B of Lancefield classification (Lancefield grouping) that can be detected directly in intact bacteria using latex agglutination tests.[7][8] The CAMP test is also another important test for identification of GBS. The CAMP factor produced by GBS acts synergistically with the staphylococcal β-hemolysin inducing enhanced hemolysis of sheep or bovine erythrocytes.[7] GBS is also able to hydrolyze hippurate and this test can also be used to identify presumptively GBS.[7] Hemolytic GBS strains produce an orange-brick-red non-isoprenoid polyene (ornithine rhamnolipid) pigment (granadaene)[9] when cultivated on granada medium that allows its straightforward identification.[10] GBS can also be identified using MALDI-TOF (Matrix Assisted Laser Desorption/Ionization-Time of Flight) instruments.[11] GBS colonies can additionally be identified tentatively after their appearance in chromogenic agar media, nevertheless GBS-like colonies that develop in chromogenic media should be confirmed as GBS using additional reliable tests (e.g.latex agglutination or the CAMP test) to avoid potential mis-identification.[8][12][13] A summary of the laboratory techniques for GBS identification is depicted in Ref 7. [8]
GBS colonization
GBS is a normal component of the intestinal and vaginal microbiota in some women, GBS is an asymptomatic (presenting no symptoms) colonizer of the gastrointestinal tract and vagina in up to 30% of otherwise healthy adults, including pregnant women.[3][14] GBS colonization may be permanent, intermittent or temporary. In different studies, GBS vaginal colonization rate ranges from 0% to 36%, most studies reporting colonization rates in sexually active women over 20%.[15] It has been estimated that maternal GBS colonization worldwide is 18%, with regional variation from 11% to 35%.[16] These variations in the reported prevalence of asymptomatic GBS colonization could be related to the detection methods used, and differences in populations sampled.[14][17]
Virulence
As other virulent bacteria, GBS harbors an important number of virulence factors (virulence factors are molecules produced by bacteria that boosts their capacity to infect and damage human tissues), the most important being the capsular polysaccharide (rich in sialic acid) [3][18] and a pore-forming toxin, β-hemolysin.[18][19][20] Today it is considered that GBS pigment and hemolysin are identical or closely related molecules.[21][22][23][24]
GBS infection in newborns
GBS colonization usually does not cause problems in healthy women, nevertheless during pregnancy it can sometimes cause serious illness for the mother and the newborn. GBS is the leading cause of bacterial neonatal infection in the baby during gestation and after delivery with significant mortality rates in premature infants. GBS infections in the mother can cause chorioamnionitis (a severe infection of the placental tissues) infrequently, postpartum infections (after birth) and it had been related with prematurity and fetal death.[25] GBS urinary tract infections (UTI) may also induce labor and cause premature delivery.[3] In the western world, GBS (in the absence of effective prevention measures) is the major cause of several bacterial infections of the newborn neonatal infection sepsis, pneumonia, and meningitis, which can lead to death or long-term sequelae.[3]
GBS neonatal infection typically originates in the lower reproductive tract of infected mothers. GBS infections in newborns are separated into two clinical syndromes, early-onset disease (EOD) and late-onset disease (LOD).[26] EOD manifests from 0 to 7 living days in the newborn, most of the cases of EOD being apparent within 24h of birth.[3][27][28] The most common clinical syndromes of EOD are sepsis without apparent focus, pneumonia, and less frequently meningitis. EOD is acquired vertically (vertical transmission), through exposure of the fetus or the baby to GBS from the vagina of a colonized woman, either intrautero or during birth after rupture of membranes. Infants can be infected during passage through the birth canal, nevertheless newborns that acquire GBS through this route can become only colonized, and these colonized infants habitually do not develop EOD. Roughly 50% of newborns to GBS colonized mothers are also GBS colonized and (without prevention measures) 1–2% of these newborns will develop EOD.[29] In the past, the incidence of EOD ranged from 0.7 to 3.7 per thousand live births in the US[3] and from 0.2 to 3.25 per thousand in Europe.[17] In 2008, after widespread use of antenatal screening and intrapartum antibiotic prophylaxis (IAP), the CDC reported an incidence of 0.28 cases of EOD per thousand live births in the US.[30]
Multistate surveillance 2006-2015 shows a decline in EOD from 0.37 to 0.23 per 1000 live births in the US but LOD remains steady at 0.31 per 1000 live births.[31]
It has been indicated that where there was a policy of providing IAP for GBS colonized mothers the overall risk of EOGBS is 0.3%.[32] Since 2006 to 2015 the incidence of GBS EOD decreased from 0.37 to 0.23 per thousand live births in the US.[33]
Though maternal GBS colonization is the key determinant for EOD, other factors also increase the risk. These factors include onset of labor before 37 weeks of gestation (premature birth), prolonged rupture of membranes (≥18h before delivery), intra-partum fever (>38 °C, >100.4 °F), amniotic infections (chorioamnionitis), young maternal age, and low levels of GBS anticapsular polysaccharide antibodies in the mother.[3][27][28] Nevertheless, most babies who develop EOD are born to GBS colonized mothers without any additional risk factor.[27][28] A previous sibling with EOD is also an important risk factor for development of the infection in subsequent deliveries, probably reflecting a lack of GBS polysaccharides protective antibodies in the mother. Heavy GBS vaginal colonization is also associated with a higher risk for EOD.[27] Overall, the case–fatality rates from EOD have declined, from 50% observed in studies from the 1970s to 2 to 10% in recent years, mainly as a consequence of improvements in therapy and management. Fatal neonatal infections by GBS are more frequent among premature infants.[3][27][28][34]
GBS LOD affects infants from 7 days to 3 months of age and is more likely to cause bacteremia or meningitis. LOD can be acquired from the mother or from environmental sources. Hearing loss and mental impairment can be a long-term sequela of GBS meningitis.[3][35][36] In contrast with EOD, the incidence of LOD has remained unchanged at 0.26 per 1000 live births in the US.[37] S. agalactiae neonatal meningitis does not present with the hallmark sign of adult meningitis, a stiff neck; rather, it presents with nonspecific symptoms, such as fever, vomiting and irritability, and can consequently lead to a late diagnosis.[2]
Prevention of neonatal infection
The only reliable way to prevent EOD currently is intrapartum antibiotic prophylaxis (IAP), that is to say administration of antibiotics during delivery. It has been proved that intravenous penicillin or ampicillin administered for at least 4 hours before delivery to GBS colonized women is very effective at preventing vertical transmission of GBS from mother to baby and EOD. Intravenous penicillin remains the agent of choice for IAP, with intravenous ampicillin as an acceptable alternative.[3][27][28] For penicillin allergic women, the laboratory requisitions for ordering antepartum GBS screening cultures should indicate clearly the presence of penicillin allergy.[28] Cefazolin, clindamycin, and vancomycin are used to prevent EOD in infants born to penicillin-allergic mothers.[27][28] Intravenous vancomycin is recommended for IAP in women colonized with a clindamycin-resistant Group B Streptococcus strain and a severe penicillin allergy.[26][28]
There are two ways to identify female candidates to receive intrapartum antibiotic prophylaxis: a risk-based approach or a culture-based screening approach. The culture-based screening approach identifies candidates to receive IAP using lower vaginal and rectal cultures obtained between 36 and 37 weeks' gestation[27][28] (32–34 weeks of gestation for women with twins[38]) and IAP is administered to all GBS colonized women. The risk-based strategy identifies candidates to receive IAP by the aforementioned risk factors known to increase the probability of EOD without considering if the mother is or is not a GBS carrier.[3][39]
IAP is also recommended for women with intrapartum risk factors if their GBS carrier status is not known at the time of delivery, for women with GBS bacteriuria during their pregnancy, and for women who have had an infant with EOD previously.
The risk-based approach for IAP is in general less effective than the culture-based approach because in most of the cases EOD develops among newborns, which are born to mothers without risk factors.[17]
In 2010, the Centers for Disease Control and Prevention (CDC), in collaboration with several professional groups, issued its revised GBS prevention guidelines.[27] In 2018, the task of revising and updating the GBS prophylaxis guidelines was transferred from the CDC to ACOG (American College of Obstetricians and Gynecologists) and the American Academy of Pediatrics. The ACOG committee issued an update document on Prevention of Group B Streptococcal Early-Onset Disease in Newborns in 2019.[28] This document does not introduce important changes from the CDC guidelines. The key measures necessary for preventing neonatal GBS early onset disease continue to be universal prenatal screening by culture of GBS from swabs collected from the lower vagina and rectum, correct collection and microbiological processing of the samples, and proper implementation of intrapartum antibiotic prophylaxis. The ACOG now recommends performing universal GBS screening between 36 and 37 weeks of gestation. This new recommendation provides a five-week window [40] for valid culture results that includes births that occur up to a gestational age of at least 41 weeks.
The culture-based screening approach is followed in most developed countries[41] such as the United States,[26][27][28] France,[42] Spain,[43] Belgium,[44] Canada, Argentina,[45] and Australia. The risk-based strategy is followed in the United Kingdom,[38][46] and the Netherlands.[17][47]
Screening for GBS colonization
Though the GBS colonization status of women can change during pregnancy, cultures to detect GBS carried out ≤5 weeks before delivery predict quite accurately the GBS carrier status at delivery. In contrast, if the prenatal culture is performed more than five weeks before delivery it is unreliable for predicting accurately the GBS carrier status at delivery.[27][28][40][48][49] The clinical specimens recommended for culture of GBS at 36–37 weeks’ gestation[28](32–34 weeks of gestation for women with twins[38]) are swabs collected the lower vagina (near the introitus) and then from the rectum (through the anal sphincter) without use of a speculum.[27][28] Following the recommendations of the Centers for Disease Control and Prevention of United States (CDC) these swabs should be placed into a non-nutritive transport medium and later inoculated into a selective enrichment broth, Todd Hewitt broth with selective antibiotics (enrichment culture).[27][50] After incubation the enrichment broth is subcultured to blood agar plates and GBS like colonies are identified by the CAMP test or using latex agglutination with GBS antisera. After incubation the enrichment broth can also be subcultured to granada medium agar[10][50] where GBS grows as pink-red colonies or to chromogenic agars, where GBS grows as colored colonies.[8][27][50] GBS-like colonies that develop in chromogenic media should be confirmed as GBS using additional reliable tests to avoid mis-identification.[8]
Nucleic acid amplification tests (NAAT) such as polymerase chain reaction (PCR) and DNA hybridization probes have been developed for identifying GBS directly from recto-vaginal samples, but they still cannot replace antenatal culture for the most accurate detection of GBS carriers.[27][28][38] Intrapartum NAAT without enrichment has a high false negative rate and the use of intrapartum NAAT without enrichment to rule out the need for IAP.[13]
_on_ChromID_CPS_chromogenic_agar_-_Detail.jpg.webp)
Vaccination
Though IAP for EOD prevention is associated with a large decline in the incidence of the disease, there is, however, no effective strategy for preventing late-onset neonatal GBS disease.[51]
Vaccination is considered an ideal solution to prevent not only EOD and LOD but also GBS infections in adults at risk.[52] Nevertheless, though research and clinical trials for the development of an effective vaccine to prevent GBS infections are underway, no vaccine was available in 2020.[53][54][55] The capsular polysaccharide of GBS is not only an important GBS virulence factor but it is also an excellent candidate for the development of an effective vaccine.[17][56][57][58] Protein-based vaccines are also in development.[53][59][55]
GBS infection in adults
GBS is also an important infectious agent able to cause invasive infections in adults. Serious life-threatening invasive GBS infections are increasingly recognized in the elderly and individuals compromised by underlying diseases such as diabetes, cirrhosis and cancer.[60] GBS infections in adults include urinary tract infection, skin and soft-tissue infection (skin and skin structure infection) bacteremia, osteomyelitis, meningitis and endocarditis.[5] GBS infection in adults can be serious and related with high mortality. In general penicillin is the antibiotic of choice for treatment of GBS infection.[61][62] Gentamicin (for synergy with penicillin G or ampicillin) can also be used in patients with life-threatening invasive GBS.[61]
Nonhuman infections
In addition to human infections, GBS is a major cause of mastitis (an infection of the udder) in dairy cattle and an important source of economic loss for the industry. GBS in cows can either produce an acute febrile disease or a subacute more chronic condition. Both lead to diminishing milk production (hence its name: agalactiae meaning "of no milk").[63] Outbreaks in herds are common, so this is of major importance for the dairy industry, and programs to reduce the impact of S. agalactiae disease have been enforced in many countries over the last 40 years.[6]
GBS also causes severe epidemics in farmed fish, causing sepsis and external and internal hemorrhages, having been reported from wild and captive fish involved in epizootics in many countries.[64][65] Vaccination is an effective method to prevent pathogenic diseases in aquaculture and different kinds vaccines to prevent GBS infections have been developed recently.[66]
GBS has also been found in many other animals, such as camels, dogs, cats, crocodiles, seals, elephants and dolphins.[67][68]
References
- Whiley RA, Hardie JM (2009). Genus I. Streptococcus Rosenbach 1884. Bergey's Manual of Systematic Bacteriology: Vol 3: The Firmicutes (2nd ed.). Springer. pp. 655–711. ISBN 978-0-387-95041-9.
- Ryan KJ, Ray CG, et al., eds. (2004). Sherris Medical Microbiology (4th ed.). McGraw Hill. pp. 286–8. ISBN 978-0-8385-8529-0.
- Edwards MS, Nizet V (2011). Group B streptococcal infections. Infectious Diseases of the Fetus and Newborn Infant (7th ed.). Elsevier. pp. 419–469. ISBN 978-0-443-06839-3.
- Slotved HC, Kong F, Lambertsen L, Sauer S, Gilbert GL (2007). "Serotype IX, a proposed new Streptococcus agalactiae serotype". J Clin Microbiol. 45 (9): 2929–2936. doi:10.1128/jcm.00117-07. PMC 2045254. PMID 17634306.
- Edwards MS, Baker CJ (2010). "Streptococcus agalactiae (group B streptococcus)". In Mandell GL, Bennett JE, Dolin R (eds.). Principles and practice of infectious diseases (7th. ed.). Elsevier. pp. Cap. 202. ISBN 978-0-443-06839-3.
- Keefe GP (1997). "Streptococcus agalactiae mastitis: a review". Can Vet J. 38 (7): 199–204. PMC 1576741. PMID 9220132.
- Tille P. (2014). Bailey & Scott's Diagnostic Microbiology (13th ed.). Elsevier. ISBN 978-0-323-08330-0.
- Rosa-Fraile M, Spellerberg B (2017). "Reliable Detection of Group B Streptococcus in the Clinical Laboratory". J Clin Microbiol. 55 (9): 2590–2598. doi:10.1128/JCM.00582-17. PMC 5648696. PMID 28659318.
- Rosa-Fraile M, Rodríguez-Granger J, Haidour-Benamin A, Cuerva JM, Sampedro A (2006). "Granadaene: Proposed Structure of the Group B Streptococcus Polyenic Pigment". Applied and Environmental Microbiology. 72 (9): 6367–6370. doi:10.1128/AEM.00756-06. PMC 1563658. PMID 16957264.CS1 maint: multiple names: authors list (link)
- Rosa-Fraile M, Rodriguez-Granger J, Cueto-Lopez M, Sampedro A, Biel Gaye E, Haro M, Andreu A (1999). "Use of Granada medium to detect group B streptococcal colonization in pregnant women". J Clin Microbiol. 37 (8): 2674–2677. doi:10.1128/JCM.37.8.2674-2677.1999. PMC 85311. PMID 10405420.
- To KN, Cornwell E, Daniel R, Goonesekera S, Jauneikaite E, Chalker V, Le Doare K (2019). "Evaluation of matrix-assisted laser desorption ionisation time-of-flight mass spectrometry (MALDI-TOF MS) for the Identification of Group B Streptococcus". BMC Res. Notes. 12 (1): 85. doi:10.1186/s13104-019-4119-1. PMC 6376729. PMID 30764872.
- El Aila NA, Tency I, Claeys G, Saerens B, Cools P, Verstraelen H, Temmerman M, Verhelst R, Vaneechoutte M (2010). "Comparison of different sampling techniques and of different culture methods for detection of group B streptococcus carriage in pregnant women". BMC Infectious Diseases. 10: 285. doi:10.1186/1471-2334-10-285. PMC 2956727. PMID 20920213.
- Filkins L, Hauser J, Robinson-Dunn Tibbetts R, Boyanton B, Revell P. "Guidelines for the Detection and Identification of Group B Streptococcus. March 10, 2020" (PDF). American Society for Microbiology. Retrieved 7 January 2021.CS1 maint: multiple names: authors list (link)
- Barcaite E, Bartusevicius A, Tameliene R, Kliucinskas M, Maleckiene L, Nadisauskiene R (2008). "Prevalence of maternal group B streptococcal colonization in European countries". Acta Obstet Gynecol Scand. 87 (3): 260–271. doi:10.1080/00016340801908759. PMID 18307064. S2CID 25897076.
- Pignanelli S, Pulcrano G, Schiavone P, Di Santo A, Zaccherini P (2015). "Selectivity evaluation of a new chromogenic medium to detect group B Streptococcus". Indian J Pathol Microbiol. 58 (1): 45–7. doi:10.4103/0377-4929.151186. PMID 25673591.
- Russell NJ, Seale AC, O'Driscoll M, O'Sullivan C, Bianchi-Jassir F, Gonzalez-Guarin J, Lawn JE, Baker CJ, Bartlett L, Cutland C, Gravett MG, Heath PT, Le Doare K, Madhi SA, Rubens CE, Schrag S, Sobanjo-Ter Meulen A, Vekemans J, Saha SK, Ip M (2017). "Maternal Colonization With Group B Streptococcus and Serotype Distribution Worldwide: Systematic Review and Meta-analyses". Clinical Infectious Diseases. 65 (Suppl 2): S100–S111. doi:10.1093/cid/cix658. PMC 5848259. PMID 29117327.
- Rodriguez-Granger J, Alvargonzalez JC, Berardi A, Berner R, Kunze M, Hufnagel M, Melin P, Decheva A, Orefici G, Poyart C, Telford J, Efstratiou A, Killian M, Krizova P, Baldassarri L, Spellerberg B, Puertas A, Rosa-Fraile M (2012). "Prevention of group B streptococcal neonatal disease revisited. The DEVANI European project". Eur J Clin Microbiol Infect Dis. 31 (9): 2097–2114. doi:10.1007/s10096-012-1559-0. PMID 22314410. S2CID 15588906.
- Rajagopal L (2009). "Understanding the regulation of Group B Streptococcal virulence factors". Future Microbiol. 4 (2): 201–221. doi:10.2217/17460913.4.2.201. PMC 2691590. PMID 19257847.
- Armistead B, Oler E, Adams Waldorf K, Rajagopal (2019). "The Double Life of Group B Streptococcus: Asymptomatic Colonizer and Potent Pathogen»". J. Mol. Biol. 431 (16): 2914–2931. doi:10.1016/j.jmb.2019.01.035. PMC 6646060. PMID 30711542.CS1 maint: multiple names: authors list (link)
- Armistead B, Whidbey C, Iyer LM, Herrero-Foncubierta P, Quach P, Haidour A, Aravind L, Cuerva JM, Jaspan HB and Rajagopal L (2020). "The cyl Genes Reveal the Biosynthetic and Evolutionary Origins of the Group B Streptococcus Hemolytic Lipid, Granadaene". Front Microbiol. 10: 3123. doi:10.3389/fmicb.2019.03123. PMC 6985545. PMID 32038561.CS1 maint: multiple names: authors list (link)
- Rosa-Fraile M, Dramsi S, Spellerberg B (2014). "Group B streptococcal haemolysin and pigment, a tale of twins" (PDF). FEMS Microbiol. Rev. 38 (5): 932–946. doi:10.1111/1574-6976.12071. PMC 4315905. PMID 24617549.
- Whidbey C, Harrell MI, Burnside K, Ngo L, Becraft AK, Iyer LM, Aravind L, Hitti J, Waldorf KM, Rajagopal L (2013). "A hemolytic pigment of Group B Streptococcus allows bacterial penetration of human placenta". J Exp Med. 210 (6): 1265–1281. doi:10.1084/jem.20122753. PMC 3674703. PMID 23712433.
- Whidbey C, Vornhagen J, Gendrin C, Boldenow E, Samson JM, Doering K, Ngo L, Ezekwe EA Jr, Gundlach JH, Elovitz MA, Liggitt D, Duncan JA, Adams Waldorf KM, Rajagopal L (2015). "A streptococcal lipid toxin induces membrane permeabilization and pyroptosis leading to fetal injury". EMBO Mol. Med. 7 (4): 488–505. doi:10.15252/emmm.201404883. PMC 4403049. PMID 25750210.
- Leclercq SY, Sullivan MJ, Ipe DS, Smith JP, Cripps AW, Ulett GC (2016). "Pathogenesis of Streptococcus urinary tract infection depends on bacterial strain and β-hemolysin/cytolysin that mediates cytotoxicity, cytokine synthesis, inflammation and virulence". Sci. Rep. 6: 29000. Bibcode:2016NatSR...629000L. doi:10.1038/srep29000. PMC 4935997. PMID 27383371.
- Muller AE, Oostvogel PM, Steegers EA, Dörr PJ (2006). "Morbidity related to maternal group B streptococcal infections". Acta Obstet Gynecol Scand. 85 (9): 1027–1037. doi:10.1080/00016340600780508. PMID 16929406. S2CID 11745321.
- Puopolo KM, Lynfield R, Cummings JJ, AAP COMMITTEE ON FETUS AND NEWBORN, AAP COMMITTEE ON INFECTIOUS DISEASES. (2019). "Management of Infants at Risk for Group B Streptococcal Disease" (PDF). Pediatrics. 144 (2): e20191881. doi:10.1542/peds.2019-1881. PMID 31285392. S2CID 195843897. Retrieved 7 January 2021.CS1 maint: multiple names: authors list (link)
- Verani JR, McGee L, Schrag SJ (2010). "Prevention of perinatal group B streptococcal disease: revised guidelines from CDC, 2010" (PDF). MMWR Recomm Rep. 59(RR-10): 1–32.
- ACOG. The American College of Obstetricians and Gynecologists (2019). "Prevention of Group B Streptococcal Early-Onset Disease in Newborns: ACOG Committee Opinion, Number 782". Obstetrics & Gynecology. 134 (1): e19–e40. doi:10.1097/AOG.0000000000003334. PMID 31241599. S2CID 195659363.
- Boyer KM, Gotoff SP (1985). "Strategies for Chemoprophylaxis of GBS Early-Onset Infections1". Strategies for chemoprophylaxis of GBS early-onset infections. Antibiot. Chemother. Antibiotics and Chemotherapy. 35. pp. 267–280. doi:10.1159/000410380. ISBN 978-3-8055-3953-1. PMID 3931544.
- CDC. "Group B Strep (GBS)-Clinical Overview". Retrieved 27 Oct 2015.
- Nanduri SA, Petit S, Smelser C, Apostol M, Alden NB, Harrison LH, Lynfield R, Vagnone PS, Burzlaff K, Spina NL, Dufort EM, Schaffner W, Thomas AR, Farley MM, Jain JH, Pondo T, McGee L, Beall BW, Schrag SJ. (2019). "Epidemiology of Invasive Early-Onset and Late-Onset Group B Streptococcal Disease in the United States, 2006 to 2015: Multistate Laboratory and Population-Based Surveillance". JAMA Pediatr. 173 (3): 224–233. doi:10.1001/jamapediatrics.2018.4826. PMC 6439883. PMID 30640366.CS1 maint: multiple names: authors list (link)
- Russell NJ, Seale AC, O'Sullivan C, Le Doare K, Heath PT, Lawn JE, Bartlett L, Cutland C, Gravett M, Ip M, Madhi SA, Rubens CE, Saha SK, Schrag S, Sobanjo-Ter Meulen A, Vekemans J, Baker CJ (2017). "Risk of Early-Onset Neonatal Group B Streptococcal Disease With Maternal Colonization Worldwide: Systematic Review and Meta-analyses". Clin Infect Dis. 65, Suppl 2 (suppl_2): S152–S159. doi:10.1093/cid/cix655. PMC 5850448. PMID 29117325.
- Nanduri SA, Petit S, Smelser C, Apostol M, Alden NB, Harrison LH, Lynfield R, Vagnone PS, Burzlaff K, Spina NL, Dufort EM, Schaffner W, Thomas AR, Farley MM, Jain JH, Pondo T, McGee L, Beall BW, Schrag SJ (2019). "Epidemiology of Invasive Early-Onset and Late-Onset Group B Streptococcal Disease in the United States, 2006 to 2015: Multistate Laboratory and Population-Based Surveillance.»". JAMA Pediatr. 173 (3): 224–233. doi:10.1001/jamapediatrics.2018.4826. PMC 6439883. PMID 30640366.
- Edmond KM, Kortsalioudaki C, Scott S, Schrag SJ, Zaidi AK, Cousens S, Heath PT (2012). "Group B streptococcal disease in infants aged younger than 3 months: systematic review and meta-analysis" (PDF). Lancet. 379 (9815): 547–556. doi:10.1016/s0140-6736(11)61651-6. PMID 22226047. S2CID 15438484.
- Libster, R; Edwards, KM; Levent, F; Edwards, MS; Rench, MA; Castagnini, LA; Cooper, T; Sparks, RC; Baker, CJ; Shah, PE (July 2012). "Long-term outcomes of group B streptococcal meningitis". Pediatrics. 130 (1): e8–15. doi:10.1542/peds.2011-3453. PMID 22689869. S2CID 1013682.
- Kohli-Lynch M, Russell NJ, Seale AC, Dangor Z, Tann CJ, Baker CJ, Bartlett L, Cutland C, Gravett MG, Heath PT, Ip M, Le Doare K, Madhi SA, Rubens CE, Saha SK, Schrag S, Sobanjo-Ter Meulen A, Vekemans J, O'Sullivan C, Nakwa F, Ben Hamouda H, Soua H, Giorgakoudi K, Ladhani S, Lamagni T, Rattue H, Trotter C, Lawn JE (2017). "Neurodevelopmental Impairment in Children After Group B Streptococcal Disease Worldwide: Systematic Review and Meta-analyses". Clinical Infectious Diseases. 65 (Suppl. 2): S190–S199. doi:10.1093/cid/cix663. PMC 5848372. PMID 29117331.
- Baker CJ (2013). "The spectrum of perinatal group B streptococcal disease". Vaccine. 31 (Suppl 4): D3–D6. doi:10.1016/j.vaccine.2013.02.030. PMID 23973344.
- Huges RG, Brocklehurst P, Steer PJ, Heath P, Stenson BM (2017). "Prevention of Early-onset Neonatal Group B Streptococcal Disease Green-top Guideline No. 36 September 2017". BJOG. Royal College of Obstetricians and Gynaecologists. 124 (12): e280–e305. doi:10.1111/1471-0528.14821. PMID 28901693.
- Clifford V, Garland SM, Grimwood K (2011). "Prevention of neonatal group B streptococcus disease in the 21st century". J Paediatr Child Health. 48 (9): 808–815. doi:10.1111/j.1440-1754.2011.02203.x. PMID 22151082. S2CID 36906520.
- Yancey MK, Schuchat A, Brown LK, Ventura VL, Markenson GR (1996). "The accuracy of late antenatal screening cultures in predicting genital group B streptococcal colonization at delivery". Obstetrics & Gynecology. 88 (5): 811–815. doi:10.1016/0029-7844(96)00320-1. PMID 8885919.
- Le Doare K, O'Driscoll M, Turner K, Seedat F, Russell NJ, Seale AC, Heath PT, Lawn JE, Baker CJ, Bartlett L, Cutland C, Gravett MG, Ip M, Madhi SA, Rubens CE, Saha SK, Schrag S, Sobanjo-Ter Meulen A, Vekemans J, Kampmann B, et al. (GBS Intrapartum Antibiotic Investigator Group) (2017). "Intrapartum Antibiotic Chemoprophylaxis Policies for the Prevention of Group B Streptococcal Disease Worldwide: Systematic Review". Clin Infect Dis. 65 (Suppl.2): S143–S151. doi:10.1093/cid/cix654. PMC 5850619. PMID 29117324.
- Agence Nationale d’Accreditation et d’Evaluation en Santé. "Prévention anténatale du risque infectieux bactérien néonatal précoce. 2001" (PDF). Retrieved 22 December 2017.
- Alós Cortés JI, Andreu Domingo A, Arribas Mir L, Cabero Roura L, Cueto Lopez M, López Sastre J, Melchor Marcos JC, Puertas Prieto A, de la Rosa Fraile M, Salcedo Abizanda S, Sánchez Luna M, Sánchez Pérez MJ, Torrejón Cardoso R (2012). "Prevención de la infección perinatal por estreptococo del grupo B. Recomendaciones españolas revisadas 2012" (PDF). Rev Esp Quimioter. 25 (1): 79–88. PMID 22488547. Retrieved 1 December 2019.
- Belgian Health Council. "PREVENTION OF PERINATAL GROUP B STREPTOCOCCAL INFECTIONS. Guidelines from the Belgian Health Council, 2003" (PDF). Retrieved 22 December 2017.
- Ministerio de Salud de la Nación. Dirección Nacional de Salud Materno Infantil. Argentina. "Recomendaciones para la prevención, diagnóstico y tratamiento de la infección neonatal precoz por Estreptococo β Hemolítico del Grupo B (EGB)" (PDF). Retrieved 2 December 2019.
- RCOG and GBSS UK. "Group B Streptococcus (GBS) in pregnancy and newborn babies" (PDF). Retrieved 7 January 2021.
- M Trijbels-Smeulders, G A de Jonge, P C M Pasker-de Jong, L J Gerards, A H Adriaanse, R A vanLingen, L A A Kolle´e (2007). "Epidemiology of neonatal group B streptococcal disease in theNetherlands before and after introduction of guidelines for prevention". Archives of Disease in Childhood - Fetal and Neonatal Edition. 92 (4): F271–F276. doi:10.1136/adc.2005.088799. PMC 2675425. PMID 17227807.CS1 maint: multiple names: authors list (link)
- Valkenburg-van den Berg AW, Houtman-Roelofsen RL, Oostvogel PM, Dekker FW, Dorr PJ, Sprij AJ (2010). "Timing of group B streptococcus screening in pregnancy: a systematic review". Gynecol Obstet. 69 (3): 174–183. doi:10.1159/000265942. PMID 20016190. S2CID 26709882.
- Virranniemi M, Raudaskoski T, Haapsamo M, Kauppila J, Renko M, Peltola J, Risteli L, Laatio L (2019). "The effect of screening-to-labor interval on the sensitivity of late-pregnancy culture in the prediction of group B streptococcus colonization at labor: A prospective multicenter cohort study". Acta Obstet Gynecol Scand. 98 (4): 494–499. doi:10.1111/aogs.13522. PMID 30578547. S2CID 58106301. Retrieved 10 January 2021.CS1 maint: multiple names: authors list (link)
- Carey RB. "Group B Streptococci: Chains & Changes New Guidelines for the Prevention of Early-Onset GBS" (PDF). Retrieved 27 Oct 2017.
- Jordan HT, Farley MM, Craig A, Mohle-Boetani J, Harrison LH, Petit S, Lynfield R, Thomas A, Zansky S, Gershman K, Albanese BA, Schaffner W, Schrag SJ (2008). "Revisiting the need for vaccine prevention of late-onset neonatal group B streptococcal disease: a multistate, population-based analysis". Pediatr Infect Dis J. 27 (12): 1057–1064. doi:10.1097/inf.0b013e318180b3b9. PMID 18989238. S2CID 1533957.
- Edwards MS, Rench MA, Rinaudo CD, Fabbrini M, Tuscano G, Buffi G, Bartolini E, Bonacci S, Baker CJ, Margarit I (2016). "Immune Responses to Invasive Group B Streptococcal Disease in Adults". Emerg Infect Dis. 22 (11): 1877–1883. doi:10.3201/eid2211.160914. PMC 5088039. PMID 27767008.
- Heath PT (2016). "Status of vaccine research and development of vaccines for GBS". Vaccine. 34 (26): 2876–2879. doi:10.1016/j.vaccine.2015.12.072. PMID 26988258.
- Davies HG, Carreras-Abad C, Le Doare K, Heath PT (2019). "Group B Streptococcus: Trials and Tribulations" (PDF). Pediatr Infect Dis J. 38 (6S Suppl 1): S72–S76. doi:10.1097/INF.0000000000002328. PMID 31205250.
- Carreras-Abad C, Ramkhelawon L, Heath PT, Le Doare K. (2020). "A Vaccine Against Group B Streptococcus: Recent Advances". Infect Drug Resist. 13: 1263–1272. doi:10.2147/IDR.S203454. PMC 7196769. PMID 32425562.CS1 maint: multiple names: authors list (link)
- Baker CJ, Carey VJ, Rench MA, Edwards MS, Hillier SH, Kasper DL, Platt R (2014). "Maternal Antibody at Delivery Protects Neonates From Early Onset Group B Streptococcal Disease" (PDF). J Infect Dis. 209 (5): 781–788. doi:10.1093/infdis/jit549. PMC 3923540. PMID 24133184.
- Edwards MS, Gonik B (2013). "Preventing the broad spectrum of perinatal morbidity and mortality throughgh group B streptococcal vaccination". Vaccine. 31S: D66–71. doi:10.1016/j.vaccine.2012.11.046. PMID 23200934.
- Madhi, Shabir A; Cutland, Clare L; Jose, Lisa; Koen, Anthonet; Govender, Niresha; Wittke, Frederick; Olugbosi, Morounfolu; Meulen, Ajoke Sobanjo-ter; Baker, Sherryl; Dull, Peter M; Narasimhan, Vas; Slobod, Karen (2016). "Safety and immunogenicity of an investigational maternal trivalent group B streptococcus vaccine in healthy women and their infants: a randomised phase 1b/2 trial". The Lancet Infectious Diseases. 16 (8): 923–934. doi:10.1016/S1473-3099(16)00152-3. ISSN 1473-3099. PMID 27139805.
- Song JY, Lim JH, Lim S, Yong Z, Seo HS (2018). "Progress toward a group B streptococcal vaccine". Hum Vaccin Immunother. 14 (11): 2669–2681. doi:10.1080/21645515.2018.1493326. PMC 6314413. PMID 29995578.
- Elena Graux, Maya Hites, Delphine Martiny, Evelyne Maillart, Marc Delforge, Pierrette Melin, Nicolas Dauby. (2020). "Invasive group B Streptococcus among non-pregnant adults in Brussels-Capital Region, 2005-2019". Eur J Clin Microbiol Infect Dis. 173 (Sep 17, 1–9): 224–233. doi:10.1007/s10096-020-04041-0. PMC 6439883. PMID 30640366.CS1 maint: multiple names: authors list (link)
- Edwards MS; . Baker CJ (2005). "Group B streptococcal infections in elderly adults". Clin Infect Dis. 41 (6): 839–847. doi:10.1086/432804. PMID 16107984.
- Farley MM (2001). "Group B Streptococcal Disease in Nonpregnant Adults" (PDF). Clinical Infectious Diseases. 33 (4): 556–561. doi:10.1086/322696. PMID 11462195.
- Ruegg PL. (2017). "A 100-Year Review: Mastitis detection, management, and prevention". J. Dairy Sci. 100 (10381–10397): 10381–10397. doi:10.3168/jds.2017-13023. PMID 29153171. Retrieved 22 November 2019.
- Evans JJ, Klesius PH, Pasnik DJ, Bohnsack JF (2009). "Human Streptococcus agalactiae isolate in Nile tilapia (Oreochromis niloticus)". Emerg Infect Dis. 15 (5): 774–776. doi:10.3201/eid1505.080222. PMC 2687030. PMID 19402966.
- Liu G, Zhang W, Lu C (2013). "Comparative genomics analysis of Streptococcus". BMC Genomics. 14: 775. doi:10.1186/1471-2164-14-775. PMC 3831827. PMID 24215651.
- Liu G, Zhu J, Chen K, Gao T, Yao H, Liu Y, Zhang W, Lu C (2016). "Development of Streptococcus agalactiae vaccines for tilapia". Dis Aquat Org. 122 (2): 163–170. doi:10.3354/dao03084. PMID 28000606.
- Delannoy CMJ, Crumlish M, Fontaine MC, Pollock J, Foster G, Dagleish MP, Turnbull JF, Zadoks RN (2013). "Human Streptococcus agalactiae strains in aquatic mammal and fish". BMC Microbiology. 13: 41. doi:10.1186/1471-2180-13-41. PMC 3585737. PMID 23419028.
- Eisenberg T, Rau J, Westerhüs U, Knauf-Witzens T, Fawzy A, Schlez K, Zschöck M, Prenger-Berninghoff E, Heydel C, Sting R, Glaeser SP, Pulami D, van der Linden M, Ewers C (2017). "Streptococcus agalactiae in elephants. A comparative study with isolates from human and zoo animal and livestock origin". Vet. Microbiol. 204: 141–150. doi:10.1016/j.vetmic.2017.04.018. PMID 28532793.