Surgery
Surgery[lower-alpha 1] is a medical or dental specialty that uses operative manual and instrumental techniques on a person to investigate or treat a pathological condition such as a disease or injury, to help improve bodily function, appearance, or to repair unwanted ruptured areas.


The act of performing surgery may be called a surgical procedure, operation, or simply "surgery". In this context, the verb "operate" means to perform surgery. The adjective surgical means pertaining to surgery; e.g. surgical instruments or surgical nurse. The person or subject on which the surgery is performed can be a person or an animal. A surgeon is a person who practices surgery and a surgeon's assistant is a person who practices surgical assistance. A surgical team is made up of the surgeon, the surgeon's assistant, an anaesthetist, a circulating nurse and a surgical technologist. Surgery usually spans from minutes to hours, but it is typically not an ongoing or periodic type of treatment. The term "surgery" can also refer to the place where surgery is performed, or, in British English, simply the office of a physician,[1] dentist, or veterinarian.
Definitions
Surgery is an invasive technique with the fundamental principle of physical intervention on organs/organ systems/tissues for diagnostic or therapeutic reasons.
As a general rule, a procedure is considered surgical when it involves cutting of a person's tissues or closure of a previously sustained wound. Other procedures that do not necessarily fall under this rubric, such as angioplasty or endoscopy, may be considered surgery if they involve "common" surgical procedure or settings, such as use of a sterile environment, anesthesia, antiseptic conditions, typical surgical instruments, and suturing or stapling. All forms of surgery are considered invasive procedures; so-called "noninvasive surgery" usually refers to an excision that does not penetrate the structure being excised (e.g. laser ablation of the cornea) or to a radiosurgical procedure (e.g. irradiation of a tumor).
Types of surgery
Surgical procedures are commonly categorized by urgency, type of procedure, body system involved, the degree of invasiveness, and special instrumentation.
- Based on timing: Elective surgery is done to correct a non-life-threatening condition, and is carried out at the person's request, subject to the surgeon's and the surgical facility's availability. A semi-elective surgery is one that must be done to avoid permanent disability or death, but can be postponed for a short time. Emergency surgery is surgery which must be done without any delay to prevent death or serious disabilties and/or loss of limbs and functions.
- Based on purpose: Exploratory surgery is performed to aid or confirm a diagnosis. Therapeutic surgery treats a previously diagnosed condition. Cosmetic surgery is done to subjectively improve the appearance of an otherwise normal structure.
- By type of procedure: Amputation involves cutting off a body part, usually a limb or digit; castration is also an example. Resection is the removal of all of an internal organ or body part, or a key part (lung lobe; liver quadrant) of such an organ or body part that has its own name or code designation. A segmental resection can be of a smaller region of an organ such as a hepatic segment or a bronchopulmonary segment.[2] Excision is the cutting out or removal of only part of an organ, tissue, or other body part from the person. Extirpation is the complete excision or surgical destruction of a body part.[3] Replantation involves reattaching a severed body part. Reconstructive surgery involves reconstruction of an injured, mutilated, or deformed part of the body. Transplant surgery is the replacement of an organ or body part by insertion of another from different human (or animal) into the person undergoing surgery. Removing an organ or body part from a live human or animal for use in transplant is also a type of surgery.
- By body part: When surgery is performed on one organ system or structure, it may be classed by the organ, organ system or tissue involved. Examples include cardiac surgery (performed on the heart), gastrointestinal surgery (performed within the digestive tract and its accessory organs), and orthopedic surgery (performed on bones or muscles).
- By degree of invasiveness of surgical procedures: Minimally-invasive surgery involves smaller outer incisions to insert miniaturized instruments within a body cavity or structure, as in laparoscopic surgery or angioplasty. By contrast, an open surgical procedure such as a laparotomy requires a large incision to access the area of interest.
- By equipment used: Laser surgery involves use of a laser for cutting tissue instead of a scalpel or similar surgical instruments. Microsurgery involves the use of an operating microscope for the surgeon to see small structures. Robotic surgery makes use of a surgical robot, such as the Da Vinci or the ZEUS robotic surgical systems, to control the instrumentation under the direction of the surgeon.
Terminology
- Excision surgery names often start with a name for the organ to be excised (cut out) and end in -ectomy.
- Procedures involving cutting into an organ or tissue end in -otomy. A surgical procedure cutting through the abdominal wall to gain access to the abdominal cavity is a laparotomy.
- Minimally invasive procedures, involving small incisions through which an endoscope is inserted, end in -oscopy. For example, such surgery in the abdominal cavity is called laparoscopy.
- Procedures for formation of a permanent or semi-permanent opening called a stoma in the body end in -ostomy.
- Reconstruction, plastic or cosmetic surgery of a body part starts with a name for the body part to be reconstructed and ends in -oplasty. Rhino is used as a prefix for "nose", therefore a rhinoplasty is reconstructive or cosmetic surgery for the nose.
- Repair of damaged or congenital abnormal structure ends in -rraphy.
- Reoperation (return to the operating room) refers to a return to the operating theater after an initial surgery is performed to re-address an aspect of patient care best treated surgically. Reasons for reoperation include persistent bleeding after surgery, development of or persistence of infection.
Description of surgical procedure
Location
Inpatient surgery is performed in a hospital, and the person undergoing surgery stays at least one night in the hospital after the surgery. Outpatient surgery occurs in a hospital outpatient department or freestanding ambulatory surgery center, and the person who had surgery is discharged the same working day.[4] Office surgery occurs in a physician's office, and the person is discharged the same working day.[5]
At a hospital, modern surgery is often performed in an operating theater using surgical instruments, an operating table, and other equipment. Among United States hospitalizations for nonmaternal and nonneonatal conditions in 2012, more than one-fourth of stays and half of hospital costs involved stays that included operating room (OR) procedures.[6] The environment and procedures used in surgery are governed by the principles of aseptic technique: the strict separation of "sterile" (free of microorganisms) things from "unsterile" or "contaminated" things. All surgical instruments must be sterilized, and an instrument must be replaced or re-sterilized if, it becomes contaminated (i.e. handled in an unsterile manner, or allowed to touch an unsterile surface). Operating room staff must wear sterile attire (scrubs, a scrub cap, a sterile surgical gown, sterile latex or non-latex polymer gloves and a surgical mask), and they must scrub hands and arms with an approved disinfectant agent before each procedure.
Preoperative care
Prior to surgery, the person is given a medical examination, receives certain pre-operative tests, and their physical status is rated according to the ASA physical status classification system. If these results are satisfactory, the person requiring surgery signs a consent form and is given a surgical clearance. If the procedure is expected to result in significant blood loss, an autologous blood donation may be made some weeks prior to surgery. If the surgery involves the digestive system, the person requiring surgery may be instructed to perform a bowel prep by drinking a solution of polyethylene glycol the night before the procedure. People preparing for surgery are also instructed to abstain from food or drink (an NPO order after midnight on the night before the procedure), to minimize the effect of stomach contents on pre-operative medications and reduce the risk of aspiration if the person vomits during or after the procedure.
Some medical systems have a practice of routinely performing chest x-rays before surgery. The premise behind this practice is that the physician might discover some unknown medical condition which would complicate the surgery, and that upon discovering this with the chest x-ray, the physician would adapt the surgery practice accordingly.[7] However, medical specialty professional organizations recommend against routine pre-operative chest x-rays for people who have an unremarkable medical history and presented with a physical exam which did not indicate a chest x-ray.[7] Routine x-ray examination is more likely to result in problems like misdiagnosis, overtreatment, or other negative outcomes than it is to result in a benefit to the person.[7] Likewise, other tests including complete blood count, prothrombin time, partial thromboplastin time, basic metabolic panel, and urinalysis should not be done unless the results of these tests can help evaluate surgical risk.[8]
Staging for surgery
The pre-operative holding area[9] is so important in the surgical phase since here is where most of the family members can see who the staff of the surgery will be, also this area is where the nurses in charge to give information to the family members of the patient. In the pre-operative holding area, the person preparing for surgery changes out of his or her street clothes and is asked to confirm the details of his or her surgery. A set of vital signs are recorded, a peripheral IV line is placed, and pre-operative medications (antibiotics, sedatives, etc.) are given.[10] When the person enters the operating room, the skin surface to be operated on, called the operating field, is cleaned and prepared by applying an antiseptic (ideally chlorhexidine gluconate in alcoholic, as this is twice as effective as povidone-iodine for reduce the risk of infection.[11] If hair is present at the surgical site, it is clipped off prior to prep application. The person is assisted by an anesthesiologist or resident to make a specific surgical position, then sterile drapes are used to cover the surgical site or at least a wide area surrounding the operating field; the drapes are clipped to a pair of poles near the head of the bed to form an "ether screen", which separates the anesthetist/anesthesiologist's working area (unsterile) from the surgical site (sterile).[12]
Anesthesia is administered to prevent pain from an incision, tissue manipulation and suturing. Depending on the kind of operation, anesthesia may be provided locally or as general anesthesia. Spinal anesthesia may be used when the surgical site is too large or deep for a local block, but general anesthesia may not be desirable. With local and spinal anesthesia, the surgical site is anesthetized, but the person can remain conscious or minimally sedated. In contrast, general anesthesia renders the person unconscious and paralyzed during surgery. The person is intubated and is placed on a mechanical ventilator, and anesthesia is produced by a combination of injected and inhaled agents. Choice of surgical method and anesthetic technique aims to reduce the risk of complications, shorten the time needed for recovery and minimise the surgical stress response.
Intraoperative phase
The intraoperative phase begins when the surgery subject is received in the surgical area (such as the operating theater or surgical department), and lasts until the subject is transferred to a recovery area (such as a post-anesthesia care unit).[13]
An incision is made to access the surgical site. Blood vessels may be clamped or cauterized to prevent bleeding, and retractors may be used to expose the site or keep the incision open. The approach to the surgical site may involve several layers of incision and dissection, as in abdominal surgery, where the incision must traverse skin, subcutaneous tissue, three layers of muscle and then the peritoneum. In certain cases, bone may be cut to further access the interior of the body; for example, cutting the skull for brain surgery or cutting the sternum for thoracic (chest) surgery to open up the rib cage. Whilst in surgery aseptic technique is used to prevent infection or further spreading of the disease. The surgeons' and assistants' hands, wrists and forearms are washed thoroughly for at least 4 minutes to prevent germs getting into the operative field, then sterile gloves are placed onto their hands. An antiseptic solution is applied to the area of the person's body that will be operated on. Sterile drapes are placed around the operative site. Surgical masks are worn by the surgical team to avoid germs on droplets of liquid from their mouths and noses from contaminating the operative site.
Work to correct the problem in body then proceeds. This work may involve:
- excision – cutting out an organ, tumor,[14] or other tissue.
- resection – partial removal of an organ or other bodily structure.
- reconnection of organs, tissues, etc., particularly if severed. Resection of organs such as intestines involves reconnection. Internal suturing or stapling may be used. Surgical connection between blood vessels or other tubular or hollow structures such as loops of intestine is called anastomosis.
- reduction – the movement or realignment of a body part to its normal position. e.g. Reduction of a broken nose involves the physical manipulation of the bone or cartilage from their displaced state back to their original position to restore normal airflow and aesthetics.
- ligation – tying off blood vessels, ducts, or "tubes".
- grafts – may be severed pieces of tissue cut from the same (or different) body or flaps of tissue still partly connected to the body but resewn for rearranging or restructuring of the area of the body in question. Although grafting is often used in cosmetic surgery, it is also used in other surgery. Grafts may be taken from one area of the person's body and inserted to another area of the body. An example is bypass surgery, where clogged blood vessels are bypassed with a graft from another part of the body. Alternatively, grafts may be from other persons, cadavers, or animals.
- insertion of prosthetic parts when needed. Pins or screws to set and hold bones may be used. Sections of bone may be replaced with prosthetic rods or other parts. Sometimes a plate is inserted to replace a damaged area of skull. Artificial hip replacement has become more common. Heart pacemakers or valves may be inserted. Many other types of prostheses are used.
- creation of a stoma, a permanent or semi-permanent opening in the body
- in transplant surgery, the donor organ (taken out of the donor's body) is inserted into the recipient's body and reconnected to the recipient in all necessary ways (blood vessels, ducts, etc.).
- arthrodesis – surgical connection of adjacent bones so the bones can grow together into one. Spinal fusion is an example of adjacent vertebrae connected allowing them to grow together into one piece.
- modifying the digestive tract in bariatric surgery for weight loss.
- repair of a fistula, hernia, or prolapse.
- repair according to the ICD-10-PCS, in the Medical and Surgical Section 0, root operation Q, means restoring, to the extent possible, a body part to its normal anatomic structure and function. This definition, repair, is used only when the method used to accomplish the repair is not one of the other root operations. Examples would be colostomy takedown, herniorrhaphy of a hernia, and the surgical suture of a laceration.
- other procedures, including:
- clearing clogged ducts, blood or other vessels
- removal of calculi (stones)
- draining of accumulated fluids
- debridement – removal of dead, damaged, or diseased tissue
Blood or blood expanders may be administered to compensate for blood lost during surgery. Once the procedure is complete, sutures or staples are used to close the incision. Once the incision is closed, the anesthetic agents are stopped or reversed, and the person is taken off ventilation and extubated (if general anesthesia was administered).[15]
Postoperative care
After completion of surgery, the person is transferred to the post anesthesia care unit and closely monitored. When the person is judged to have recovered from the anesthesia, he/she is either transferred to a surgical ward elsewhere in the hospital or discharged home. During the post-operative period, the person's general function is assessed, the outcome of the procedure is assessed, and the surgical site is checked for signs of infection. There are several risk factors associated with postoperative complications, such as immune deficiency and obesity. Obesity has long been considered a risk factor for adverse post-surgical outcomes. It has been linked to many disorders such as obesity hypoventilation syndrome, atelectasis and pulmonary embolism, adverse cardiovascular effects, and wound healing complications.[16] If removable skin closures are used, they are removed after 7 to 10 days post-operatively, or after healing of the incision is well under way.
It is not uncommon for surgical drains (see Drain (surgery)) to be required to remove blood or fluid from the surgical wound during recovery. Mostly these drains stay in until the volume tapers off, then they are removed. These drains can become clogged, leading to abscess.
Postoperative therapy may include adjuvant treatment such as chemotherapy, radiation therapy, or administration of medication such as anti-rejection medication for transplants. Other follow-up studies or rehabilitation may be prescribed during and after the recovery period.
The use of topical antibiotics on surgical wounds to reduce infection rates has been questioned.[17] Antibiotic ointments are likely to irritate the skin, slow healing, and could increase risk of developing contact dermatitis and antibiotic resistance.[17] It has also been suggested that topical antibiotics should only be used when a person shows signs of infection and not as a preventative.[17] A systematic review published by Cochrane (organisation) in 2016, though, concluded that topical antibiotics applied over certain types of surgical wounds reduce the risk of surgical site infections, when compared to no treatment or use of antiseptics.[18] The review also did not find conclusive evidence to suggest that topical antibiotics increased the risk of local skin reactions or antibiotic resistance.
Through a retrospective analysis of national administrative data, the association between mortality and day of elective surgical procedure suggests a higher risk in procedures carried out later in the working week and on weekends. The odds of death were 44% and 82% higher respectively when comparing procedures on a Friday to a weekend procedure. This "weekday effect" has been postulated to be from several factors including poorer availability of services on a weekend, and also, decrease number and level of experience over a weekend.[19]
While pain is universal and expected after surgery, there is growing evidence that pain may be inadequately treated in many people in the acute period immediately after surgery. It has been reported that incidence of inadequately controlled pain after surgery ranged from 25.1% to 78.4% across all surgical disciplines.[20]
Postoperative recovery has been defined as an energy‐requiring process to decrease physical symptoms, reach a level of emotional well‐being, regain functions, and re‐establish activities.[21] Moreover, it has been identified that patients who have undergone surgery are often not fully recovered on discharge.
Epidemiology
United States
In 2011, of the 38.6 million hospital stays in U.S. hospitals, 29% included at least one operating room procedure. These stays accounted for 48% of the total $387 billion in hospital costs.[22]
The overall number of procedures remained stable from 2001 to 2011. In 2011, over 15 million operating room procedures were performed in U.S. hospitals.[23]
Data from 2003 to 2011 showed that U.S. hospital costs were highest for the surgical service line; the surgical service line costs were $17,600 in 2003 and projected to be $22,500 in 2013.[24] For hospital stays in 2012 in the United States, private insurance had the highest percentage of surgical expenditure.[25] in 2012, mean hospital costs in the United States were highest for surgical stays.[25]
Special populations
Elderly people
Older adults have widely varying physical health. Frail elderly people are at significant risk of post-surgical complications and the need for extended care. Assessment of older people before elective surgery can accurately predict the person's recovery trajectories.[26] One frailty scale uses five items: unintentional weight loss, muscle weakness, exhaustion, low physical activity, and slowed walking speed. A healthy person scores 0; a very frail person scores 5. Compared to non-frail elderly people, people with intermediate frailty scores (2 or 3) are twice as likely to have post-surgical complications, spend 50% more time in the hospital, and are three times as likely to be discharged to a skilled nursing facility instead of to their own homes.[26] People who are frail and elderly (score of 4 or 5) have even worse outcomes, with the risk of being discharged to a nursing home rising to twenty times the rate for non-frail elderly people.
Children
Surgery on children requires considerations that are not common in adult surgery. Children and adolescents are still developing physically and mentally making it difficult for them to make informed decisions and give consent for surgical treatments. Bariatric surgery in youth is among the controversial topics related to surgery in children.
Vulnerable populations
Doctors perform surgery with the consent of the person undergoing surgery. Some people are able to give better informed consent than others. Populations such as incarcerated persons, people living with dementia, the mentally incompetent, persons subject to coercion, and other people who are not able to make decisions with the same authority as others, have special needs when making decisions about their personal healthcare, including surgery.
'Global Surgery' in low- and middle-income countries
Surgery remains grossly neglected in global health, famously described by Halfdan T. Mahler as the 'neglected stepchild of global health'. This particularly affects low-resource settings with weak surgical health systems. 'Global surgery' is the term now adopted to describe the rapidly developing field seeking to address this, and has been defined as 'the multidisciplinary enterprise of providing improved and equitable surgical care to the world's population, with its core tenets as the issues of need, access and quality'.[27]
In 2014, The Lancet Commission on Global Surgery was launched to examine the case for surgery as an integral component of global health care and to provide recommendations regarding the delivery of surgical and anesthesia services in low and middle income countries.[28] In this study, two primary conclusions were reached:
- Five billion people worldwide lack access to safe, timely, and affordable surgical and anesthesia care. Areas in which especially large proportions of the population lack access include Sub-Saharan Africa, the Indian Subcontinent, Central Asia and, to a lesser extent, Russia and China. Of the estimated 312.9 million surgical procedures undertaken worldwide in 2012, only 6.3% were done in countries comprising the poorest 37.3% of the world's population.
- An additional 143 million surgical procedures are needed each year to prevent unnecessary death and disability.
Globally, 4.2 million people are estimated to die within 30 days of surgery each year, with half of these occurring in low- and middle-income countries.[29] A prospective study of 10,745 adults undergoing emergency abdominal surgery from 357 centres across 58 countries found that mortality is three times higher in low- compared with high-human development index (HDI) countries even when adjusted for prognostic factors.[30] In this study the overall global mortality rate was 1·6 per cent at 24 hours (high HDI 1·1 per cent, middle HDI 1·9 per cent, low HDI 3·4 per cent), increasing to 5·4 per cent by 30 days (high HDI 4·5 per cent, middle HDI 6·0 per cent, low HDI 8·6 per cent; P < 0·001). A sub-study of 1,409 children undergoing emergency abdominal surgery from 253 centres across 43 countries found that adjusted mortality in children following surgery may be as high as 7 times greater in low-HDI and middle-HDI countries compared with high-HDI countries. This translates to 40 excess deaths per 1000 procedures performed in these settings.[31] Patient safety factors were suggested to play an important role, with use of the WHO Surgical Safety Checklist associated with reduced mortality at 30 days.[32]
Introducing novel or new surgical techniques in low- and middle-income countries is a challenge.[33] Challenges include knowledge (awareness), fear, costs, and cultural beliefs.[34]
Human rights
Access to surgical care is increasingly recognized as an integral aspect of healthcare, and therefore is evolving into a normative derivation of human right to health.[35] The ICESCR Article 12.1 and 12.2 define the human right to health as "the right of everyone to the enjoyment of the highest attainable standard of physical and mental health"[36] In the August 2000, the UN Committee on Economic, Social and Cultural Rights (CESCR) interpreted this to mean "right to the enjoyment of a variety of facilities, goods, services, and conditions necessary for the realization of the highest attainable health".[37] Surgical care can be thereby viewed as a positive right – an entitlement to protective healthcare.[37]
Woven through the International Human and Health Rights literature is the right to be free from surgical disease. The 1966 ICESCR Article 12.2a described the need for "provision for the reduction of the stillbirth-rate and of infant mortality and for the healthy development of the child"[38] which was subsequently interpreted to mean "requiring measures to improve… emergency obstetric services".[37] Article 12.2d of the ICESCR stipulates the need for "the creation of conditions which would assure to all medical service and medical attention in the event of sickness",[39] and is interpreted in the 2000 comment to include timely access to "basic preventative, curative services… for appropriate treatment of injury and disability.".[40] Obstetric care shares close ties with reproductive rights, which includes access to reproductive health.[40]
Surgeons and public health advocates, such as Kelly McQueen, have described surgery as "Integral to the right to health".[41] This is reflected in the establishment of the WHO Global Initiative for Emergency and Essential Surgical Care in 2005,[42] the 2013 formation of the Lancet Commission for Global Surgery,[43] the 2015 World Bank Publication of Volume 1 of its Disease Control Priorities "Essential Surgery",[44] and the 2015 World Health Assembly 68.15 passing of the Resolution for Strengthening Emergency and Essential Surgical Care and Anesthesia as a Component of Universal Health Coverage.[45] The Lancet Commission for Global Surgery outlined the need for access to "available, affordable, timely and safe" surgical and anesthesia care;[46] dimensions paralleled in ICESCR General Comment No. 14, which similarly outlines need for available, accessible, affordable and timely healthcare.[37]
History
Trepanation
Surgical treatments date back to the prehistoric era. The oldest for which there is evidence is trepanation,[47] in which a hole is drilled or scraped into the skull, thus exposing the dura mater in order to treat health problems related to intracranial pressure and other diseases.
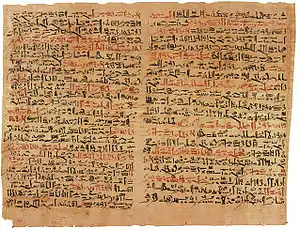
Ancient Egypt
Prehistoric surgical techniques are seen in Ancient Egypt, where a mandible dated to approximately 2650 BC shows two perforations just below the root of the first molar, indicating the draining of an abscessed tooth. Surgical texts from ancient Egypt date back about 3500 years ago. Surgical operations were performed by priests, specialized in medical treatments similar to today,[48] and used sutures to close wounds.[49] Infections were treated with honey.[50]
India

Remains from the early Harappan periods of the Indus Valley Civilization (c. 3300 BC) show evidence of teeth having been drilled dating back 9,000 years.[51] Susruta[52] was an ancient Indian surgeon commonly credited as the author of the treatise Sushruta Samhita. He is well known as the "father of surgery", and his period is usually placed around 1200–600 BC.[53] One of the earliest known mentions of the name is from the Bower Manuscript, in which Sushruta is listed as one of the ten sages residing in the Himalayas.[54] Texts suggest that he learned surgery at Kasi from Lord Dhanvantari, the god of medicine in Hindu mythology.[55] It is one of the oldest known surgical texts and it describes in detail the examination, diagnosis, treatment, and prognosis of numerous ailments, as well as procedures for various forms of cosmetic surgery, plastic surgery and rhinoplasty.[56]
Ancient Greece
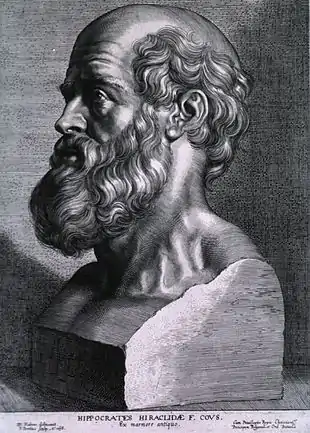
In ancient Greece, temples dedicated to the healer-god Asclepius, known as Asclepieia (Greek: Ασκληπιεία, sing. Asclepieion Ασκληπιείον), functioned as centers of medical advice, prognosis, and healing.[57] In the Asclepieion of Epidaurus, some of the surgical cures listed, such as the opening of an abdominal abscess or the removal of traumatic foreign material, are realistic enough to have taken place.[15] The Greek Galen was one of the greatest surgeons of the ancient world and performed many audacious operations – including brain and eye surgery – that were not tried again for almost two millennia.
Researchers from the Adelphi University discovered in the Paliokastro on Thasos ten skeletal remains, four women and six men, who were buried between the fourth and seventh centuries A.D. Their bones illuminated their physical activities, traumas, and even a complex form of brain surgery. According to the researchers: "The very serious trauma cases sustained by both males and females had been treated surgically or orthopedically by a very experienced physician/surgeon with great training in trauma care. We believe it to have been a military physician". The researchers were impressed by the complexity of the brain surgical operation.[58]
Islamic World
During the Islamic Golden Age, largely based upon Paul of Aegina's Pragmateia, the writings of Abulcasis (Abu al-Qasim Khalaf ibn al-Abbas Al-Zahrawi), an Andalusian-Arab physician and scientist who practiced in the Zahra suburb of Córdoba, were influential.[59][60] Al-Zahrawi specialized in curing disease by cauterization. He invented several surgical instruments for purposes such as inspection of the interior of the urethra and for removing foreign bodies from the throat, the ear, and other body organs. He was also the first to illustrate the various cannulae and to treat warts with an iron tube and caustic metal as a boring instrument. He describes what is thought to be the first attempt at reduction mammaplasty for the management of gynaecomastia[61] and the first mastectomy to treat breast cancer.[62] He is credited with the performance of the first thyroidectomy.[63] Al-Zahrawi pioneered techniques of neurosurgery and neurological diagnosis, treating head injuries, skull fractures, spinal injuries, hydrocephalus, subdural effusions and headache. The first clinical description of an operative procedure for hydrocephalus was given by Al-Zahrawi, who clearly describes the evacuation of superficial intracranial fluid in hydrocephalic children.[64]
Early modern Europe


In Europe, the demand grew for surgeons to formally study for many years before practicing; universities such as Montpellier, Padua and Bologna were particularly renowned. In the 12th century, Rogerius Salernitanus composed his Chirurgia, laying the foundation for modern Western surgical manuals. Barber-surgeons generally had a bad reputation that was not to improve until the development of academic surgery as a specialty of medicine, rather than an accessory field.[65] Basic surgical principles for asepsis etc., are known as Halsteads principles.
There were some important advances to the art of surgery during this period. The professor of anatomy at the University of Padua, Andreas Vesalius, was a pivotal figure in the Renaissance transition from classical medicine and anatomy based on the works of Galen, to an empirical approach of 'hands-on' dissection. In his anatomic treaties De humani corporis fabrica, he exposed the many anatomical errors in Galen and advocated that all surgeons should train by engaging in practical dissections themselves.
The second figure of importance in this era was Ambroise Paré (sometimes spelled "Ambrose"[66]), a French army surgeon from the 1530s until his death in 1590. The practice for cauterizing gunshot wounds on the battlefield had been to use boiling oil; an extremely dangerous and painful procedure. Paré began to employ a less irritating emollient, made of egg yolk, rose oil and turpentine. He also described more efficient techniques for the effective ligation of the blood vessels during an amputation.
Modern surgery
The discipline of surgery was put on a sound, scientific footing during the Age of Enlightenment in Europe. An important figure in this regard was the Scottish surgical scientist, John Hunter, generally regarded as the father of modern scientific surgery.[67] He brought an empirical and experimental approach to the science and was renowned around Europe for the quality of his research and his written works. Hunter reconstructed surgical knowledge from scratch; refusing to rely on the testimonies of others, he conducted his own surgical experiments to determine the truth of the matter. To aid comparative analysis, he built up a collection of over 13,000 specimens of separate organ systems, from the simplest plants and animals to humans.
He greatly advanced knowledge of venereal disease and introduced many new techniques of surgery, including new methods for repairing damage to the Achilles tendon and a more effective method for applying ligature of the arteries in case of an aneurysm.[68] He was also one of the first to understand the importance of pathology, the danger of the spread of infection and how the problem of inflammation of the wound, bone lesions and even tuberculosis often undid any benefit that was gained from the intervention. He consequently adopted the position that all surgical procedures should be used only as a last resort.[69]
Other important 18th- and early 19th-century surgeons included Percival Pott (1713–1788) who described tuberculosis on the spine and first demonstrated that a cancer may be caused by an environmental carcinogen (he noticed a connection between chimney sweep's exposure to soot and their high incidence of scrotal cancer). Astley Paston Cooper (1768–1841) first performed a successful ligation of the abdominal aorta, and James Syme (1799–1870) pioneered the Symes Amputation for the ankle joint and successfully carried out the first hip disarticulation.
Modern pain control through anesthesia was discovered in the mid-19th century. Before the advent of anesthesia, surgery was a traumatically painful procedure and surgeons were encouraged to be as swift as possible to minimize patient suffering. This also meant that operations were largely restricted to amputations and external growth removals. Beginning in the 1840s, surgery began to change dramatically in character with the discovery of effective and practical anaesthetic chemicals such as ether, first used by the American surgeon Crawford Long, and chloroform, discovered by Scottish obstetrician James Young Simpson and later pioneered by John Snow, physician to Queen Victoria.[70] In addition to relieving patient suffering, anaesthesia allowed more intricate operations in the internal regions of the human body. In addition, the discovery of muscle relaxants such as curare allowed for safer applications.
Infection and antisepsis
Unfortunately, the introduction of anesthetics encouraged more surgery, which inadvertently caused more dangerous patient post-operative infections. The concept of infection was unknown until relatively modern times. The first progress in combating infection was made in 1847 by the Hungarian doctor Ignaz Semmelweis who noticed that medical students fresh from the dissecting room were causing excess maternal death compared to midwives. Semmelweis, despite ridicule and opposition, introduced compulsory handwashing for everyone entering the maternal wards and was rewarded with a plunge in maternal and fetal deaths; however, the Royal Society dismissed his advice.
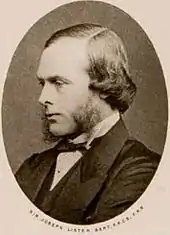
Until the pioneering work of British surgeon Joseph Lister in the 1860s, most medical men believed that chemical damage from exposures to bad air (see "miasma") was responsible for infections in wounds, and facilities for washing hands or a patient's wounds were not available.[71] Lister became aware of the work of French chemist Louis Pasteur, who showed that rotting and fermentation could occur under anaerobic conditions if micro-organisms were present. Pasteur suggested three methods to eliminate the micro-organisms responsible for gangrene: filtration, exposure to heat, or exposure to chemical solutions. Lister confirmed Pasteur's conclusions with his own experiments and decided to use his findings to develop antiseptic techniques for wounds. As the first two methods suggested by Pasteur were inappropriate for the treatment of human tissue, Lister experimented with the third, spraying carbolic acid on his instruments. He found that this remarkably reduced the incidence of gangrene and he published his results in The Lancet.[72] Later, on 9 August 1867, he read a paper before the British Medical Association in Dublin, on the Antiseptic Principle of the Practice of Surgery, which was reprinted in The British Medical Journal.[73][74][75] His work was groundbreaking and laid the foundations for a rapid advance in infection control that saw modern antiseptic operating theatres widely used within 50 years.
Lister continued to develop improved methods of antisepsis and asepsis when he realised that infection could be better avoided by preventing bacteria from getting into wounds in the first place. This led to the rise of sterile surgery. Lister introduced the Steam Steriliser to sterilize equipment, instituted rigorous hand washing and later implemented the wearing of rubber gloves. These three crucial advances – the adoption of a scientific methodology toward surgical operations, the use of anaesthetic and the introduction of sterilised equipment – laid the groundwork for the modern invasive surgical techniques of today.
The use of X-rays as an important medical diagnostic tool began with their discovery in 1895 by German physicist Wilhelm Röntgen. He noticed that these rays could penetrate the skin, allowing the skeletal structure to be captured on a specially treated photographic plate.
 Hieronymus Fabricius, Operationes chirurgicae, 1685
Hieronymus Fabricius, Operationes chirurgicae, 1685 John Syng Dorsey wrote the first American textbook on surgery
John Syng Dorsey wrote the first American textbook on surgery An operation in 1753, painted by Gaspare Traversi.
An operation in 1753, painted by Gaspare Traversi.
Surgical specialties
- General surgery
- Breast
- Cardiothoracic
- Colorectal
- Craniofacial surgery
- Dental surgery
- Endocrine
- Gynaecology
- Neurosurgery
- Ophthalmology
- Oncological
- Oral and maxillofacial surgery
- Transplant
- Orthopaedic surgery
- Hand surgery
- Otolaryngology
- Paediatric (Pediatric)
- Plastic
- Podiatric surgery
- Skin
- Trauma
- Urology
- Vascular
Learned societies
- World Federation of Neurosurgical Societies
- American College of Surgeons
- American College of Osteopathic Surgeons
- American Academy of Orthopedic Surgeons
- American College of Foot and Ankle Surgeons
- Royal Australasian College of Surgeons
- Royal Australasian College of Dental Surgeons
- Royal College of Physicians and Surgeons of Canada
- Royal College of Surgeons in Ireland
- Royal College of Surgeons of Edinburgh
- Royal College of Physicians and Surgeons of Glasgow
- Royal College of Surgeons of England
See also
- Anesthesia – State of medically-controlled temporary loss of sensation or awareness
- ASA physical status classification system
- Biomaterial – Any substance that has been engineered to interact with biological systems for a medical purpose
- Cardiac surgery
- Current Procedural Terminology (CPT) – Medical coding used in the United States – for outpatient surgical procedures medical coding
- Surgical drain – Tube used to remove pus, blood or other fluids from a wound
- Endoscopy
- Fluorescence image-guided surgery
- Hypnosurgery
- Healthcare Cost and Utilization Project (HCUP) – a family of health care databases etc. from the US
- ICD-10 Procedure Coding System – International system of medical classification used for procedural coding (International Classification of Diseases, 10th edition, Procedural Coding System; inpatient surgical procedures medical coding)
- Jet ventilation
- List of surgical procedures
- Minimally invasive procedure
- Operative report
- Perioperative mortality
- Physician Assistant
- Remote surgery
- Robot-assisted surgery – Surgical procedure
- Surgeon's assistant
- Surgical Outcomes Analysis and Research
- Surgical sieve
- Trauma surgery
- Reconstructive surgery
- Rheumasurgery
- WHO Surgical Safety Checklist
Notes
References
- "Doctor's surgery". Collins English Dictionary. Archived from the original on 10 February 2018. Retrieved 10 February 2018.
- "NCI Dictionary of Cancer Terms - National Cancer Institute". www.cancer.gov. 2 February 2011. Retrieved 31 July 2020.
- "extirpation". Merriam-Webster dictionary. Retrieved 20 February 2020.
- Lemos P, Jarrett P, Philip B, eds. (2006). Day surgery: development and practice (PDF). London: International Association for Ambulatory Surgery. ISBN 978-989-20-0234-7.
- Twersky RS, Philip BK, eds. (2008). Handbook of ambulatory anesthesia (2nd ed.). New York: Springer. p. 284. ISBN 978-0-387-73328-9.
- Fingar KR, Stocks C, Weiss AJ, Steiner CA (December 2014). "Most Frequent Operating Room Procedures Performed in U.S. Hospitals, 2003–2012". HCUP Statistical Brief No. 186. Rockville, MD: Agency for Healthcare Research and Quality. Archived from the original on 3 May 2015.
- American College of Radiology. "Five Things Physicians and Patients Should Question". Choosing Wisely: An Initiative of the ABIM Foundation. Archived from the original on 10 February 2013. Retrieved 17 August 2012., citing
- "American College of Radiology ACR Appropriateness Criteria". American College of Radiology. 2000. Archived from the original on 10 February 2013. Retrieved 4 September 2012. Last reviewed 2011.
- Gómez-Gil, E.; Trilla, A.; Corbella, B.; Fernández-Egea, E.; Luburich, P.; De Pablo, J.; Ferrer Raldúa, J.; Valdés, M. (2002). "Lack of clinical relevance of routine chest radiography in acute psychiatric admissions". General Hospital Psychiatry. 24 (2): 110–13. doi:10.1016/s0163-8343(01)00179-7. PMID 11869746.
- Archer, C.; Levy, A.R.; McGregor, M. (1993). "Value of routine preoperative chest x-rays: A meta-analysis". Canadian Journal of Anesthesia. 40 (11): 1022–27. doi:10.1007/BF03009471. PMID 8269561.
- Munro, J.; Booth, A.; Nicholl, J. (1997). "Routine preoperative testing: A systematic review of the evidence". Health Technology Assessment (Winchester, England). 1 (12): i–iv, 1–62. doi:10.3310/hta1120. PMID 9483155.
- Grier, D.J.; Watson, L.J.; Hartnell, G.G.; Wilde, P. (1993). "Are routine chest radiographs prior to angiography of any value?". Clinical Radiology. 48 (2): 131–33. doi:10.1016/S0009-9260(05)81088-8. PMID 8004892.
- Gupta, S.D.; Gibbins, F.J.; Sen, I. (1985). "Routine chest radiography in the elderly". Age and Ageing. 14 (1): 11–14. doi:10.1093/ageing/14.1.11. PMID 4003172.
- Amorosa JK; Bramwit MP; Mohammed TL; Reddy GP; et al. "ACR Appropriateness Criteria routine chest radiographs in ICU patients". National Guideline Clearinghouse. Archived from the original on 15 September 2012. Retrieved 4 September 2012.
- American Society for Clinical Pathology, "Five Things Physicians and Patients Should Question", Choosing Wisely: an initiative of the ABIM Foundation, American Society for Clinical Pathology, archived from the original on 1 September 2013, retrieved 1 August 2013, which cites
- Keay, L; Lindsley, K; Tielsch, J; Katz, J; Schein, O (8 January 2019). "Routine preoperative medical testing for cataract surgery". The Cochrane Database of Systematic Reviews. 1: CD007293. doi:10.1002/14651858.CD007293.pub4. PMC 6353242. PMID 30616299.
- Katz, R.I.; Dexter, F.; Rosenfeld, K.; Wolfe, L.; Redmond, V.; Agarwal, D.; Salik, I.; Goldsteen, K.; Goodman, M.; Glass, P.S.A. (2011). "Survey Study of Anesthesiologistsʼ and Surgeonsʼ Ordering of Unnecessary Preoperative Laboratory Tests". Anesthesia & Analgesia. 112 (1): 207–12. doi:10.1213/ANE.0b013e31820034f0. PMID 21081771. S2CID 8480050.
- Munro, J.; Booth, A.; Nicholl, J. (1997). "Routine preoperative testing: A systematic review of the evidence". Health Technology Assessment (Winchester, England). 1 (12): i–iv, 1–62. doi:10.3310/hta1120. PMID 9483155.
- Reynolds, T.M.; National Institute for Health Clinical Excellence; Clinical Science Reviews Committee of the Association for Clinical Biochemistry (2006). "National Institute for Health and Clinical Excellence guidelines on preoperative tests: The use of routine preoperative tests for elective surgery". Annals of Clinical Biochemistry. 43 (Pt 1): 13–16. doi:10.1258/000456306775141623. PMID 16390604.
- Capdenat Saint-Martin, E.; Michel, P.; Raymond, J.M.; Iskandar, H.; Chevalier, C.; Petitpierre, M.N.; Daubech, L.; Amouretti, M.; Maurette, P. (1998). "Description of local adaptation of national guidelines and of active feedback for rationalising preoperative screening in patients at low risk from anaesthetics in a French university hospital". Quality in Health Care. 7 (1): 5–11. doi:10.1136/qshc.7.1.5. PMC 2483578. PMID 10178152.
- Dunn, D. (1997). Responsibilities of the preoperative holding area nurse. AORN journal, 66(5), 819-838.
- "The day of your surgery – adult: MedlinePlus Medical Encyclopedia". medlineplus.gov. Retrieved 24 January 2019.
- Wade, Ryckie G.; Burr, Nicholas E.; McCauley, Gordon; Bourke, Grainne; Efthimiou, Orestis (1 September 2020). "The Comparative Efficacy of Chlorhexidine Gluconate and Povidone-iodine Antiseptics for the Prevention of Infection in Clean Surgery: A Systematic Review and Network Meta-analysis". Annals of Surgery. Publish Ahead of Print. doi:10.1097/SLA.0000000000004076. PMID 32773627.
- Martin, Shirley (2007). Minor Surgical Procedures for Nurses and Allied Healthcare Professionals. England: John Wiley & Sons, Ltd. p. 122. ISBN 978-0-470-01990-0.
- Page 2 in: Spry, Cynthia (2009). Essentials of perioperative nursing. Sudbury, Mass: Jones and Bartlett Publishers. ISBN 978-0-7637-5881-3. OCLC 227920274.
- Wagman LD. "Principles of Surgical Oncology" Archived 15 May 2009 at the Wayback Machine in Pazdur R, Wagman LD, Camphausen KA, Hoskins WJ (Eds) Cancer Management: A Multidisciplinary Approach Archived 4 October 2013 at the Wayback Machine. 11 ed. 2008.
- Askitopoulou, H., Konsolaki, E., Ramoutsaki, I., Anastassaki, E. Surgical cures by sleep induction as the Asclepieion of Epidaurus. The history of anesthesia: proceedings of the Fifth International Symposium, by José Carlos Diz, Avelino Franco, Douglas R. Bacon, J. Rupreht, Julián Alvarez. Elsevier Science B.V., International Congress Series 1242(2002), pp. 11–17.
- Doyle S.L.; Lysaght J.; Reynolds J.V. (2010). "Obesity and post-operative complications in patients undergoing non-bariatric surgery". Obesity Reviews. 11 (12): 875–86. doi:10.1111/j.1467-789X.2009.00700.x. PMID 20025695. S2CID 7712323.
- American Academy of Dermatology (February 2013), "Five Things Physicians and Patients Should Question", Choosing Wisely: an initiative of the ABIM Foundation, American Academy of Dermatology, archived from the original on 1 December 2013, retrieved 5 December 2013, which cites
- Sheth, V.M.; Weitzul, S. (2008). "Postoperative topical antimicrobial use". Dermatitis : Contact, Atopic, Occupational, Drug. 19 (4): 181–89. doi:10.2310/6620.2008.07094. PMID 18674453.
- Heal, Clare F; Banks, Jennifer L; Lepper, Phoebe D; Kontopantelis, Evangelos; van Driel, Mieke L (2016). "Topical antibiotics for preventing surgical site infection in wounds healing by primary intention" (PDF). Cochrane Database of Systematic Reviews. 11: CD011426. doi:10.1002/14651858.cd011426.pub2. PMC 6465080. PMID 27819748. Archived from the original (PDF) on 23 July 2018. Alt URL
- Aylin P, Alexandrescu R, Jen MH, Mayer EK, Bottle A (2013). "Day of week of procedure and 30-day mortality for elective surgery: retrospective analysis of hospital episode statistics". BMJ. 346: f2424. doi:10.1136/bmj.f2424. PMC 3665889. PMID 23716356.
- Yang, Michael M H; Hartley, Rebecca L; Leung, Alexander A; Ronksley, Paul E; Jetté, Nathalie; Casha, Steven; Riva-Cambrin, Jay (April 2019). "Preoperative predictors of poor acute postoperative pain control: a systematic review and meta-analysis". BMJ Open. 9 (4): e025091. doi:10.1136/bmjopen-2018-025091. ISSN 2044-6055. PMC 6500309. PMID 30940757.
- Allvin, Renée; Berg, Katarina; Idvall, Ewa; Nilsson, Ulrica (March 2007). "Postoperative recovery: a concept analysis". Journal of Advanced Nursing. 57 (5): 552–558. doi:10.1111/j.1365-2648.2006.04156.x. ISSN 0309-2402. PMID 17284272.
- Weiss AJ, Elixhauser A, Andrews RM (February 2014). "Characteristics of Operating Room Procedures in U.S. Hospitals, 2011". HCUP Statistical Brief No. 170. Rockville, MD: Agency for Healthcare Research and Quality. Archived from the original on 28 March 2014.
- Weiss AJ, Elixhauser A (March 2014). "Trends in Operating Room Procedures in U.S. Hospitals, 2001–2011". HCUP Statistical Brief No. 171. Rockville, MD: Agency for Healthcare Research and Quality. Archived from the original on 28 March 2014.
- Weiss AJ, Barrett ML, Steiner CA (July 2014). "Trends and Projections in Inpatient Hospital Costs and Utilization, 2003–2013". HCUP Statistical Brief No. 175. Rockville, MD: Agency for Healthcare Research and Quality. Archived from the original on 3 August 2014.
- Moore B, Levit K, Elixhauser A (October 2014). "Costs for Hospital Stays in the United States, 2012". HCUP Statistical Brief No. 181. Rockville, MD: Agency for Healthcare Research and Quality. Archived from the original on 29 November 2014.
- Makary MA, Segev DL, Pronovost PJ, et al. (June 2010). "Frailty as a predictor of surgical in older patients". J. Am. Coll. Surg. 210 (6): 901–08. doi:10.1016/j.jamcollsurg.2010.01.028. PMID 20510798. Lay summary (28 December 2010).
- Bath M, Bashford T, Fitzgerald JE (2019). "What is 'global surgery'? Defining the multidisciplinary interface between surgery, anaesthesia and public health". BMJ Global Health. 4 (5): e001808. doi:10.1136/bmjgh-2019-001808. PMC 6830053. PMID 31749997.
- Meara JG, Leather AJ, Hagander L, Alkire BC, Alonso N (2015). "Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development". Lancet. 386 (9993): 569–624. doi:10.1016/S0140-6736(15)60160-X. PMID 25924834. S2CID 2048403.
- Bhangu, Aneel; Morton, Dion G.; Brocklehurst, Peter; Lilford, Richard; Garden, O. James; Yepez, Raul; Verjee, Azmina; Tabiri, Stephen; Sundar, Sudha (2 February 2019). "Global burden of postoperative death". The Lancet. 393 (10170): 401. doi:10.1016/S0140-6736(18)33139-8. ISSN 0140-6736. PMID 30722955.
- GlobalSurg Collaborative (2016). "Mortality of emergency abdominal surgery in high-, middle- and low-income countries". British Journal of Surgery. 103 (8): 971–988. doi:10.1002/bjs.10151. hdl:20.500.11820/7c4589f5-7845-4405-a384-dfb5653e2163. PMID 27145169. S2CID 20764511.
- GlobalSurg Collaborative (2016). "Determinants of morbidity and mortality following emergency abdominal surgery in children in low-income and middle-income countries". BMJ Global Health. 1 (4): e000091. doi:10.1136/bmjgh-2016-000091. PMC 5321375. PMID 28588977.
- GlobalSurg Collaborative (2016). "Mortality of emergency abdominal surgery in high-, middle- and low-income countries". British Journal of Surgery. 103 (8): 971–988. doi:10.1002/bjs.10151. hdl:20.500.11820/7c4589f5-7845-4405-a384-dfb5653e2163. PMID 27145169. S2CID 20764511.
- Bolton, W. S.; Aruparayil, N.; Quyn, A.; Scott, J.; Wood, A.; Bundu, I.; Gnanaraj, J.; Brown, J. M.; Jayne, D. G. (2019). "Disseminating technology in global surgery". BJS. 106 (2): e34–e43. doi:10.1002/bjs.11036. ISSN 0007-1323. PMID 30620068.
- Schecter, William P.; Adhikari, Sweta (2015), Debas, Haile T.; Donkor, Peter; Gawande, Atul; Jamison, Dean T. (eds.), "Global Surgery and Poverty", Essential Surgery: Disease Control Priorities, Third Edition (Volume 1), The International Bank for Reconstruction and Development / The World Bank, pp. 353–359, doi:10.1596/978-1-4648-0346-8_ch20, ISBN 9781464803468, PMID 26740997, retrieved 8 August 2019
- Marks S. Normative Expansion of the Right to Health and the Proliferation of Human Rights. George Washington International Law Review. 2016:101–44
- UN General Assembly. International Covenant on Economic, Social and Cultural Rights – United Nations Treaty Series. In: Nations U, editor. 1966
- UN Committee on Economic Social and Cultural Rights. CESCR General Comment No. 14: The Right to the Highest Attainable Standard of Health (Art. 12) 2000
- UN General Assembly. International Covenant on Economic, Social and Cultural Rights – United Nations Treaty Series. In: Nations U, editor. 1966.
- 2. UN General Assembly. International Covenant on Economic, Social and Cultural Rights – United Nations Treaty Series. In: Nations U, editor. 1966.
- UN Committee on Economic Social and Cultural Rights. CESCR General Comment No. 14: The Right to the Highest Attainable Standard of Health (Art. 12) 2000.
- McQueen KA, Ozgediz D, Riviello R, Hsia RY, Jayaraman S, Sullivan SR; et al. (June 2010). ""Essential surgery " Integral to the right to health". Health and Human Rights. 12 (1): 137–52. PMID 20930260.CS1 maint: multiple names: authors list (link)
- World Health Organization. Global Initiative for Emergency and Essential Surgical Care 2017 [cited 2017 October 23rd]. Available from: "WHO | WHO Global Initiative for Emergency and Essential Surgical Care". Archived from the original on 25 March 2012. Retrieved 9 February 2012.
- Meara JG, Leather AJ, Hagander L, Alkire BC, Alonso N, Ameh EA; et al. (April 2015). "Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development". International Journal of Obstetric Anesthesia. 25: 75–8. doi:10.1016/j.ijoa.2015.09.006. PMID 26597405.CS1 maint: multiple names: authors list (link)
- Debas HT, Donker P, Gawande A, Jamison DT, Kruk ME, Mock CN, editors. Essential Surgery. Disease Control Priorities. 3rd ed. Washington, DC: International Bank for Reconstruction and Development / World Bank Group; 2015
- Price R, Makasa E, Hollands M (September 2015). "World Health Assembly Resolution WHA68.15: "Strengthening Emergency and Essential Surgical Care and Anesthesia as a Component of Universal Health Coverage"-Addressing the Public Health Gaps Arising from Lack of Safe, Affordable and Accessible Surgical and Anesthetic Services". World J. Surg. 39 (9): 2115–25. doi:10.1007/s00268-015-3153-y. PMID 26239773. S2CID 13027859.CS1 maint: multiple names: authors list (link)
- Meara JG, Leather AJ, Hagander L, Alkire BC, Alonso N, Ameh EA; et al. (April 2015). "Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development". International Journal of Obstetric Anesthesia. 25: 75–78. doi:10.1016/j.ijoa.2015.09.006. PMID 26597405.CS1 maint: multiple names: authors list (link)
- Capasso, Luigi (2002). Principi di storia della patologia umana: corso di storia della medicina per gli studenti della Facoltà di medicina e chirurgia e della Facoltà di scienze infermieristiche (in Italian). Rome: SEU. ISBN 978-88-87753-65-3. OCLC 50485765.
- Shiffman, Melvin (2012). Cosmetic Surgery: Art and Techniques. Springer. p. 20. ISBN 978-3-642-21837-8.
- Sullivan R (1996). "The Identity and Work of the Ancient Egyptian Surgeon". Journal of the Royal Society of Medicine. 89 (8): 467–73. doi:10.1177/014107689608900813. PMC 1295891. PMID 8795503.
- James P. Allen, The Art of Medicine in Ancient Egypt. (New York: The Metropolitan Museum of Art, 2005) 72.
- "Stone age man used dentist drill". BBC News. 6 April 2006. Archived from the original on 22 April 2009. Retrieved 24 May 2010.
- Monier-Williams, A Sanskrit Dictionary (1899)
- Singh, P.B.; Pravin S. Rana (2002). Banaras Region: A Spiritual and Cultural Guide. Varanasi: Indica Books. p. 31. ISBN 978-81-86569-24-5.
- Kutumbian, pp. xxxii–xxxiii
- Monier-Williams, A Sanskrit Dictionary, s.v. "suśruta"
- History of plastic surgery in India. Rana RE, Arora BS, – J Postgrad Med Archived 1 March 2009 at the Wayback Machine
- Risse, G.B. Mending bodies, saving souls: a history of hospitals. Oxford University Press, 1990. p. 56
- Adelphi researcher discovers early, complex brain surgery in ancient Greece
- Zimmerman, Leo M.; Veith, Ilza (1993). Great Ideas in the History of Surgery. Norman Publishing. pp. 82–83. ISBN 978-0-930405-53-3. Retrieved 3 December 2012.
- Pormann, Peter E. (2004). The Oriental Tradition of Paul of Aegina's Pragmateia. Brill. pp. 300–04. ISBN 978-90-04-13757-8. Retrieved 6 December 2012.
- Ahmad, Z. (St Thomas' Hospital) (2007), "Al-Zahrawi – The Father of Surgery", ANZ Journal of Surgery, 77 (Suppl. 1): A83, doi:10.1111/j.1445-2197.2007.04130_8.x, S2CID 57308997
- "Pioneer Muslim Physicians". aramcoworld.com. Archived from the original on 21 March 2017. Retrieved 20 March 2017.
- Ignjatovic M: Overview of the history of thyroid surgery. Acta Chir Iugosl 2003; 50: 9–36.
- Aschoff, A.; Kremer, P.; Hashemi, B.; Kunze, S. (October 1999). "The scientific history of hydrocephalus and its treatment". Neurosurgical Review. 22 (2–3): 67–93, discussion 94–95. doi:10.1007/s101430050035. ISSN 0344-5607. PMID 10547004. S2CID 10077885.
- Sven Med Tidskr. (2007). "From barber to surgeon – the process of professionalization". Svensk Medicinhistorisk Tidskrift. 11 (1): 69–87. PMID 18548946.
- Levine JM (March 1992). "Historical notes on pressure ulcers: the cure of Ambrose Paré". Decubitus. 5 (2): 23–24, 26. PMID 1558689.
- Moore, Wendy (2005). The Knife Man: The Extraordinary Life and Times of John Hunter, Father of Modern Surgery. Crown Publishing Group. ISBN 978-0-7679-1652-3. Retrieved 7 February 2013.
- "John Hunter: "the father of scientific surgery": Resources from the collection of the P.I. Nixon Library". Archived from the original on 26 October 2013. Retrieved 17 December 2012.
- "John Hunter: 'Founder of Scientific Surgery'". Archived from the original on 14 December 2013. Retrieved 17 December 2012.
- Gordon, H. Laing (2002). Sir James Young Simpson and Chloroform (1811–1870). The Minerva Group, Inc. p. 108. ISBN 978-1-4102-0291-8. Retrieved 11 November 2011.
- Robinson, Victor (2005). The Story of Medicine. Kessinger Publishing. p. 420. ISBN 978-1-4191-5431-7.
- The Lancet, "On a new method of treating compound fracture, abscess, etc.: with observation on the conditions of suppuration".
Five articles running from:
Volume 89, Issue 2272, 16 March 1867, pp. 326–29 (Originally published as Volume 1, Issue 2272)
to:
Volume 90, Issue 2291, 27 July 1867, pp. 95–96 Originally published as Volume 2, Issue 2291 - Lister J (21 September 1867). "On the Antiseptic Principle in the Practice of Surgery". The British Medical Journal. 2 (351): 245–60. doi:10.1136/bmj.2.351.246. PMC 2310614. PMID 20744875.. Reprinted in Lister, BJ (2010). "The classic: On the antiseptic principle in the practice of surgery. 1867". Clinical Orthopaedics and Related Research. 468 (8): 2012–16. doi:10.1007/s11999-010-1320-x. PMC 2895849. PMID 20361283.
- Lister, Joseph. "Modern History Sourcebook: Joseph Lister (1827–1912): Antiseptic Principle Of The Practice Of Surgery, 1867". Fordham University. Archived from the original on 7 November 2011. Retrieved 2 September 2011.Modernized version of text
- Lister, Joseph (December 2007). On the Antiseptic Principle of the Practice of Surgery by Baron Joseph Lister. Project Gutenberg. Archived from the original on 9 October 2011. Retrieved 2 September 2011. E-text, audio at Project Gutenberg.