Angiography
Angiography or arteriography is a medical imaging technique used to visualize the inside, or lumen, of blood vessels and organs of the body, with particular interest in the arteries, veins, and the heart chambers. This is traditionally done by injecting a radio-opaque contrast agent into the blood vessel and imaging using X-ray based techniques such as fluoroscopy.
| Angiography | |
|---|---|
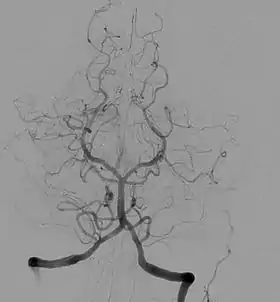 Angiogram showing a transverse projection of the vertebrobasilar and posterior cerebral circulation. | |
| ICD-9-CM | 88.40-88.68 |
| MeSH | D000792 |
| OPS-301 code | 3–60 |
The word itself comes from the Greek words ἀγγεῖον angeion, "vessel", and γράφειν graphein, "to write" or "record". The film or image of the blood vessels is called an angiograph, or more commonly an angiogram. Though the word can describe both an arteriogram and a venogram, in everyday usage the terms angiogram and arteriogram are often used synonymously, whereas the term venogram is used more precisely.[1]
The term angiography has been applied to radionuclide angiography and newer vascular imaging techniques such as CO2 angiography, CT angiography and MR angiography.[2] The term isotope angiography has also been used, although this more correctly is referred to as isotope perfusion scanning.
History
The technique was first developed in 1927 by the Portuguese physician and neurologist Egas Moniz at the University of Lisbon to provide contrasted x-ray cerebral angiography in order to diagnose several kinds of nervous diseases, such as tumors, artery disease and arteriovenous malformations. Moniz is recognized as the pioneer in this field.[3] He performed the first cerebral angiogram in Lisbon in 1927, and Reynaldo dos Santos performed the first aortogram in the same city in 1929. In fact, many current angiography techniques were developed by the Portuguese at the University of Lisbon. For example, in 1932, Lopo de Carvalho performed the first pulmonary angiogram via venous puncture of the superior member; in 1948 the first cavogram was performed by Sousa Pereira. Radial access technique for angiography can be traced back to 1953, where Eduardo Pereira first cannulated the radial artery to perform a coronary angiogram. With the introduction of the Seldinger technique in 1953, the procedure became markedly safer as no sharp introductory devices needed to remain inside the vascular lumen.
Technique
Depending on the type of angiogram, access to the blood vessels is gained most commonly through the femoral artery, to look at the left side of the heart and at the arterial system; or the jugular or femoral vein, to look at the right side of the heart and at the venous system. Using a system of guide wires and catheters, a type of contrast agent (which shows up by absorbing the X-rays), is added to the blood to make it visible on the X-ray images.
The X-ray images taken may either be still, displayed on an image intensifier or film, or motion images. For all structures except the heart, the images are usually taken using a technique called digital subtraction angiography or DSA. Images in this case are usually taken at 2–3 frames per second, which allows the interventional radiologist to evaluate the flow of the blood through a vessel or vessels. This technique "subtracts" the bones and other organs so only the vessels filled with contrast agent can be seen. The heart images are taken at 15–30 frames per second, not using a subtraction technique. Because DSA requires the patient to remain motionless, it cannot be used on the heart. Both these techniques enable the interventional radiologist or cardiologist to see stenosis (blockages or narrowings) inside the vessel which may be inhibiting the flow of blood and causing pain.
After the procedure has been completed, if the femoral technique is applied, the site of arterial entry is either manually compressed, stapled shut, or sutured in order to prevent access-site complications.[4]

Uses

Coronary angiography
One of the most common angiograms performed is to visualize the blood in the coronary arteries. A long, thin, flexible tube called a catheter is used to administer the X-ray contrast agent at the desired area to be visualized. The catheter is threaded into an artery in the forearm, and the tip is advanced through the arterial system into the major coronary artery. X-ray images of the transient radiocontrast distribution within the blood flowing inside the coronary arteries allows visualization of the size of the artery openings. The presence or absence of atherosclerosis or atheroma within the walls of the arteries cannot be clearly determined.
Coronary angiography can visualize coronary artery stenosis, or narrowing of the blood vessel. The degree of stenosis can be determined by comparing the width of the lumen of narrowed segments of blood vessel with wider segments of adjacent vessel.[4]
To detect coronary artery disease, a CT scan is more satisfactory than an MRI scan. The sensitivity and specificity between CT and MRI were (97.2 percent and 87.4 percent) and (87.1 percent and 70.3 percent), respectively. Therefore, CT (mainly multislice CT) is more accepted, more widely available, more favored by patients, and more economic. Moreover, CT requires shorter breath-hold time than MRI.[5]
Fluorescein angiography
Fluorescein angiography is a medical procedure in which a fluorescent dye is injected into the bloodstream. The dye highlights the blood vessels in the back of the eye so they can be photographed. This test is often used to manage eye disorders.[6]
OCT angiography
Optical coherence tomography (OCT) is a technology using near-infrared light to image the eye, in particular penetrate the retina to view the micro-structure behind the retinal surface. ocular OCT angiography (OCTA) is a method leveraging OCT technology to assess the vascular health of the retina.[7]
Microangiography
Microangiography is commonly used to visualize tiny blood vessels.
Neuro-vascular angiography
Another increasingly common angiographic procedure is neuro-vascular digital subtraction angiography in order to visualise the arterial and venous supply to the brain. Intervention work such as coil-embolisation of aneurysms and AVM gluing can also be performed.
Peripheral angiography
Angiography is also commonly performed to identify vessels narrowing in patients with leg claudication or cramps, caused by reduced blood flow down the legs and to the feet; in patients with renal stenosis (which commonly causes high blood pressure) and can be used in the head to find and repair stroke. These are all done routinely through the femoral artery, but can also be performed through the brachial or axillary (arm) artery. Any stenoses found may be treated by the use of balloon angioplasty, stenting, or atherectomy.
Post mortem CT angiography for medicolegal cases
Post mortem CT angiography for medicolegal cases is a method initially developed by the Virtopsy group. Originating from that project, both watery[8] and oily[9] solutions have been evaluated.
While oily solutions[9] require special deposition equipment to collect waste water, watery[8] solutions seem to be regarded as less problematic. Watery solutions also were documented to enhance post mortem CT tissue differentiation whereas oily solutions were not. Conversely, oily solutions seem to only minimally disturb ensuing toxicological analysis, while watery solutions may significantly impede toxicological analysis, thus requiring blood sample preservation before post mortem CT angiography.[10]
Complications
After an angiogram, a sudden shock can cause a little pain at the surgery area, but heart attacks and strokes usually don't occur, as they may in bypass surgery. A heart attack occurs when blood flow to a part of the heart is blocked, usually by a blood clot. Without oxygenated blood, the heart muscle begins to die. A stroke is a brain attack, cutting off vital blood flow and oxygen to the brain. Stroke happens when a blood vessel feeding the brain gets clogged or bursts.
Cerebral angiography
Major complications in cerebral angiography such as in digital subtraction angiography or contrast MRI are also rare but include stroke, an allergic reaction to the anaesthetic other medication or the contrast medium, blockage or damage to one of the access veins in the leg, or thrombosis and embolism formation. Bleeding or bruising at the site where the contrast is injected are minor complications, delayed bleeding can also occur but is rare.[11]
Additional risks
The contrast medium that is used usually produces a sensation of warmth lasting only a few seconds, but may be felt in a greater degree in the area of injection. If the patient is allergic to the contrast medium, much more serious side effects are inevitable; however, with new contrast agents the risk of a severe reaction is less than one in 80,000 examinations. Additionally, damage to blood vessels can occur at the site of puncture/injection, and anywhere along the vessel during passage of the catheter. If digital subtraction angiography is used instead, the risks are considerably reduced because the catheter does not need to be passed as far into the blood vessels; thus lessening the chances of damage or blockage.
See also
- Angiosarcoma
- Cardiac catheterization
- Computed tomography angiography
- Contrast medium
- Echocardiogram
- Electrocardiogram
- Fluorescein angiography
- Image intensifier
- Interventional radiology
- Intravascular ultrasound
- Intravenous digital subtraction angiography
- Magnetic resonance angiography
- Peripheral artery occlusive disease
References
- G. Timothy Johnson, M.D. (1986-01-23). "Arteriograms, Venograms Are Angiogram Territory". Chicago Tribune. Retrieved 12 September 2011.
- Martin, Elizabeth (2015). "Angiography". Concise Medical Dictionary (9th ed.). Oxford: Oxford University Press. doi:10.1093/acref/9780199687817.001.0001. ISBN 9780199687817.
- Berrios GE (March 1997). "The origins of psychosurgery: Shaw, Burckhardt and Moniz". History of Psychiatry. 8 (29 pt 1): 61–81. doi:10.1177/0957154X9700802905. PMID 11619209.
- Masters, Barry R. (2012-05-25). Harrisons's Principles of Internal Medicine, 18th Edition, two volumes and DVD. Eds: Dan L. Longo, Anthony S. Fauci, Dennis L. Kasper, Stephen L. Hauser, J. Larry Jameson and Joseph Loscalzo. Graefe's Archive for Clinical and Experimental Ophthalmology. 250. McGraw Hill. pp. 1407–1408. doi:10.1007/s00417-012-1940-9. ISBN 9780071748896. ISSN 0721-832X.
- "CT more accurate than MRI for ruling out coronary artery disease". February 1, 2010.
- "Fluorescein Angiography". EMPIRE RETINA CONSULTANTS. Retrieved 22 August 2016.
- Kashani AH, Chen CL, Gahm JK, Zheng F, Richter GM, Rosenfeld PJ, Shi Y, Wang RK (September 2017). "Optical coherence tomography angiography: A comprehensive review of current methods and clinical applications". Progress in Retinal and Eye Research. 60: 66–100. doi:10.1016/j.preteyeres.2017.07.002. PMC 5600872. PMID 28760677.
- Ross S, Spendlove D, Bolliger S, Christe A, Oesterhelweg L, Grabherr S, Thali MJ, Gygax E (2008). "Postmortem whole-body CT angiography: evaluation of two contrast media solutions". AJR Am. J. Roentgenol. 190 (5): 1380–9. doi:10.2214/AJR.07.3082. PMID 18430859.
- Grabherr S, Djonov V, Friess A, Thali MJ, Ranner G, Vock P, Dirnhofer R (2006). "Postmortem angiography after vascular perfusion with diesel oil and a lipophilic contrast agent". AJR Am. J. Roentgenol. 187 (5): W515–23. doi:10.2214/AJR.05.1394. PMID 17056884.
- Rutty GN, Smith P, Visser T, Barber J, Amorosa J, Morgan B (2012). "The effect on toxicology, biochemistry and immunology investigations by the use of targeted post-mortem computed tomography angiography". Forensic Sci. Int. 225 (1–3): 42–7. doi:10.1016/j.forsciint.2012.05.012. PMID 22704555.
- "Angiography – Complications". Health A-Z. NHS Choices. 2009-06-01. Retrieved 2010-03-24.
External links
| Wikimedia Commons has media related to Angiography. |
- RadiologyInfo for patients: Angiography procedures
- Cardiac Catheterization from Angioplasty.Org
- C-Arms types Several types of C-Arms
- Angiography Equipment from Siemens Medical
- Cardiovascular and Interventional Radiological Society of Europe
- Coronary CT angiography by Eugene Lin
| X-ray/ Radiography | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MRI | |||||||||||||
| Ultrasound | |||||||||||||
| Radionuclide |
| ||||||||||||
| Optical/Laser | |||||||||||||
| Thermography |
| ||||||||||||
| Target conditions | |||||||||||||
| |||||||||||||