Medical cannabis
Medical cannabis, or medical marijuana (MMJ), is cannabis and cannabinoids that are prescribed by physicians for their patients.[1][2] The use of cannabis as medicine has not been rigorously tested due to production and governmental restrictions, resulting in limited clinical research to define the safety and efficacy of using cannabis to treat diseases.[3] Preliminary evidence suggests that cannabis can reduce nausea and vomiting during chemotherapy, improve appetite in people with HIV/AIDS, and reduce chronic pain and muscle spasms.[4][5][6]
| Part of a series on |
| Cannabis |
|---|
 |
|
Short-term use increases the risk of minor and major adverse effects.[5] Common side effects include dizziness, feeling tired, vomiting, and hallucinations.[5] Long-term effects of cannabis are not clear.[5] Concerns include memory and cognition problems, risk of addiction, schizophrenia in young people, and the risk of children taking it by accident.[4]
The Cannabis plant has a history of medicinal use dating back thousands of years in many cultures.[7] Some American medical organizations have requested removal of cannabis from the list of Schedule I controlled substances maintained by the United States federal government, followed by regulatory and scientific review.[8][9] Others oppose its legalization, such as the American Academy of Pediatrics.[10]
Medical cannabis can be administered through various methods, including capsules, lozenges, tinctures, dermal patches, oral or dermal sprays, cannabis edibles, and vaporizing or smoking dried buds. Synthetic cannabinoids are available for prescription use in some countries, such as dronabinol and nabilone. Countries that allow the medical use of whole-plant cannabis include Australia, Canada, Chile, Colombia, Germany, Greece, Israel, Italy, the Netherlands, Peru, Poland, Portugal, and Uruguay. In the United States, 33 states and the District of Columbia have legalized cannabis for medical purposes, beginning with the passage of California's Proposition 215 in 1996.[11] Although cannabis remains prohibited for any use at the federal level, the Rohrabacher–Farr amendment was enacted in December 2014, limiting the ability of federal law to be enforced in states where medical cannabis has been legalized.
Classification
The National Institute on Drug Abuse defines medical cannabis as "using the whole, unprocessed marijuana plant or its basic extracts to treat symptoms of illness and other conditions".[12]
A Cannabis plant includes more than 400 different chemicals, of which about 70 are cannabinoids.[13] In comparison, typical government-approved medications contain only one or two chemicals.[13] The number of active chemicals in cannabis is one reason why treatment with cannabis is difficult to classify and study.[13]
A 2014 review stated that the variations in ratio of CBD-to-THC in botanical and pharmaceutical preparations determines the therapeutic vs psychoactive effects (CBD attenuates THC's psychoactive effects[14]) of cannabis products.[15]
Medical uses
.jpg.webp)
Overall research into the health effects of medical cannabis has been of low quality and it is not clear whether it is a useful treatment for any condition, or whether harms outweight any benefit.[16] There is no consistent evidence that it helps with chronic pain and muscle spasms.[16] Low quality evidence suggests its use for reducing nausea during chemotherapy, improving appetite in HIV/AIDS, improving sleep, and improving tics in Tourette syndrome.[5] When usual treatments are ineffective, cannabinoids have also been recommended for anorexia, arthritis, glaucoma,[17] and migraine.[18] It is unclear whether American states might be able to mitigate the adverse effects of the opioid epidemic by prescribing medical cannabis as an alternative pain management drug.[19]
It is recommended that cannabis use be stopped in pregnancy.[20]
Nausea and vomiting
Medical cannabis is somewhat effective in chemotherapy-induced nausea and vomiting (CINV)[4][17] and may be a reasonable option in those who do not improve following preferential treatment.[21] Comparative studies have found cannabinoids to be more effective than some conventional antiemetics such as prochlorperazine, promethazine, and metoclopramide in controlling CINV,[22] but these are used less frequently because of side effects including dizziness, dysphoria, and hallucinations.[23][24] Long-term cannabis use may cause nausea and vomiting, a condition known as cannabinoid hyperemesis syndrome (CHS).[25]
A 2016 Cochrane review said that cannabinoids were "probably effective" in treating chemotherapy-induced nausea in children, but with a high side-effect profile (mainly drowsiness, dizziness, altered moods, and increased appetite). Less common side effects were "ocular problems, orthostatic hypotension, muscle twitching, pruritus, vagueness, hallucinations, lightheadedness and dry mouth".[26]
HIV/AIDS
Evidence is lacking for both efficacy and safety of cannabis and cannabinoids in treating patients with HIV/AIDS or for anorexia associated with AIDS. As of 2013, current studies suffer from the effects of bias, small sample size, and lack of long-term data.[27]
Pain
Research into the use of cannabis for treating chronic pain has yielded inconsistent results for neuropathic pain, spasms associated with multiple sclerosis and pain from rheumatic disorders. Cannabis is not effective at treating chronic cancer pain.[16]
When cannabis is inhaled to relieve pain, blood levels of cannabinoids rise faster than when oral products are used, peaking within three minutes and attaining an analgesic effect in seven minutes.[28]
A 2011 review considered cannabis to be generally safe,[29] and it appears safer than opioids in palliative care.[30]
Neurological conditions
Cannabis' efficacy is not clear in treating neurological problems, including multiple sclerosis (MS) and movement problems.[15] Evidence also suggests that oral cannabis extract is effective for reducing patient-centered measures of spasticity.[15] A trial of cannabis is deemed to be a reasonable option if other treatments have not been effective.[4] Its use for MS is approved in ten countries.[4][31] A 2012 review found no problems with tolerance, abuse, or addiction.[32] In the United States, cannabidiol, one of the cannabinoids found in the marijuana plant, has been approved for treating two severe forms of epilepsy, Lennox-Gastaut syndrome and Dravet syndrome.[33]
Posttraumatic stress disorder
There is no good evidence that medical cannabis is effective for treating posttraumatic stress disorder, and its use for this purpose is not recommended.[34]
Adverse effects
.jpg.webp)
Medical use
There is insufficient data to draw strong conclusions about the safety of medical cannabis.[35] Typically, adverse effects of medical cannabis use are not serious;[4] they include tiredness, dizziness, increased appetite, and cardiovascular and psychoactive effects. Other effects can include impaired short-term memory; impaired motor coordination; altered judgment; and paranoia or psychosis at high doses.[36] Tolerance to these effects develops over a period of days or weeks. The amount of cannabis normally used for medicinal purposes is not believed to cause any permanent cognitive impairment in adults, though long-term treatment in adolescents should be weighed carefully as they are more susceptible to these impairments. Withdrawal symptoms are rarely a problem with controlled medical administration of cannabinoids. The ability to drive vehicles or to operate machinery may be impaired until a tolerance is developed.[21] Although supporters of medical cannabis say that it is safe,[35] further research is required to assess the long-term safety of its use.[23][37]
Recreational use
Tetrahydrocannabinol (THC), the principal psychoactive constituent of the cannabis plant, has low toxicity while the LD50 (dose of THC needed to kill 50% of tested rodents) is high. Acute effects may include anxiety and panic, impaired attention, and memory (while intoxicated), an increased risk of psychotic symptoms, and possibly increased risk of accidents if a person drives a motor vehicle while intoxicated.[38] Psychotic episodes are well-documented and typically resolve within minutes or hours. There have been few reports of symptoms lasting longer.[39][40]
According to the United States Department of Health and Human Services, there were 455,000 emergency room visits associated with cannabis use in 2011. These statistics include visits in which the patient was treated for a condition induced by or related to recent cannabis use. The drug use must be "implicated" in the emergency department visit, but does not need to be the direct cause of the visit. Most of the illicit drug emergency room visits involved multiple drugs.[41] In 129,000 cases, cannabis was the only implicated drug.[42][43]
Effects of chronic use may include bronchitis, a cannabis dependence syndrome, and subtle impairments of attention and memory. These deficits persist while chronically intoxicated.[38] Compared to non-smokers, people who smoked cannabis regularly in adolescence exhibit reduced connectivity in specific brain regions associated with memory, learning, alertness, and executive function.[43] One study suggested that sustained heavy, daily, adolescent onset cannabis use over decades is associated with a decline in IQ by age 38, with no effects found in those who initiated cannabis use later, or in those who ceased use earlier in adulthood.[44] A follow-up review found that IQ deficit may be a precursor, rather than result, of cannabis use, and that social and environmental factors are a likely influence.[45]
There has been a limited amount of studies that have looked at the effects of smoking cannabis on the respiratory system.[46] Chronic heavy marijuana smoking is associated with coughing, production of sputum, wheezing, coughing, and other symptoms of chronic bronchitis.[38] Regular cannabis use has not been shown to cause significant abnormalities in lung function.[47]
Cannabis smoke contains thousands of organic and inorganic chemical compounds. This tar is chemically similar to that found in tobacco smoke,[48] and over fifty known carcinogens have been identified in cannabis smoke,[49] including nitrosamines, reactive aldehydes, and polycyclic hydrocarbons, including benz[a]pyrene.[50] Light and moderate use of cannabis is not believed to increase risk of lung or upper airway cancer. Evidence for causing these cancers is mixed concerning heavy, long-term use. In general there are far lower risks of pulmonary complications for regular cannabis smokers when compared with those of tobacco.[47] Combustion products are not present when using a vaporizer, consuming THC in pill form, or consuming cannabis edibles.
There is serious suspicion among cardiologists, spurring research but falling short of definitive proof, that cannabis use has the potential to contribute to cardiovascular disease.[51] Cannabis is believed to be an aggravating factor in rare cases of arteritis, a serious condition that in some cases leads to amputation. Because 97% of case-reports also smoked tobacco, a formal association with cannabis could not be made. If arteritis turns out to be a distinct clinical entity, it might be the consequence of vasoconstrictor activity observed from delta-8-THC and delta-9-THC.[52] Other serious cardiovascular events including myocardial infarction, stroke, sudden cardiac death, and cardiomyopathy have been reported to be temporally associated with cannabis use. Research in these events is complicated because cannabis is often used in conjunction with tobacco, and drugs such as alcohol and cocaine.[53] These putative effects can be taken in context of a wide range of cardiovascular phenomena regulated by the endocannabinoid system and an overall role of cannabis in causing decreased peripheral resistance and increased cardiac output, which potentially could pose a threat to those with cardiovascular disease.[54]
Cannabis usually causes no tolerance or withdrawal symptoms except in heavy users. In a survey of heavy users 42.4% experienced withdrawal symptoms when they tried to quit marijuana such as craving, irritability, boredom, anxiety and sleep disturbances.[55] About 9% of those who experiment with marijuana eventually become dependent. The rate goes up to one in six among those who begin use as adolescents, and one-quarter to one-half of those who use it daily according to a NIDA review.[43] A 2013 review estimates daily use is associated with a 10-20% rate of dependence.[4] The highest risk of cannabis dependence is found in those with a history of poor academic achievement, deviant behavior in childhood and adolescence, rebelliousness, poor parental relationships, or a parental history of drug and alcohol problems.[56]
A 2013 literature review found that exposure to marijuana had biologically-based physical, mental, behavioral and social health consequences and was "associated with diseases of the liver (particularly with co-existing hepatitis C), lungs, heart, and vasculature".[57] There are numerous other reasons why people look for medical cannabis and to make people aware of whether they are eligible to accept medical cannabis as a dose, there are numerous websites that are currently providing online consultations through video calling. People are provided licenses with the help of which, they can either grow medical cannabis, or purchase it legally throughout the state. This is done only after precisely reviewing the applications of patients.[58]
Cognitive effects
A 2011 systematic review evaluated published studies of the acute and long-term cognitive effects of cannabis. THC intoxication is well established to impair cognitive functioning on an acute basis, including effects on the ability to plan, organize, solve problems, make decisions, and control impulses. The extent of this impact may be greater in novice users, and paradoxically, those habituated to high-level ingestion may have reduced cognition during withdrawal. Studies of long-term effects on cognition have provided conflicting results, with some studies finding no difference between long-term abstainers and never-users and others finding long-term deficits. The discrepancies between studies may reflect greater long-term effects among heavier users relative to occasional users, and greater duration of effect among those with heavy use as adolescents compared to later in life.[59] A second systematic review focused on neuroimaging studies found little evidence supporting an effect of cannabis use on brain structure and function.[60] A 2003 meta-analysis concluded that any long-term cognitive effects were relatively modest in magnitude and limited to certain aspects of learning and memory.[61]
Impact on psychosis
Exposure to THC can cause acute transient psychotic symptoms in healthy individuals and people with schizophrenia.[14]
A 2007 meta analysis concluded that cannabis use reduced the average age of onset of psychosis by 2.7 years relative to non-cannabis use.[62] A 2005 meta analysis concluded that adolescent use of cannabis increases the risk of psychosis, and that the risk is dose-related.[63] A 2004 literature review on the subject concluded that cannabis use is associated with a two-fold increase in the risk of psychosis, but that cannabis use is "neither necessary nor sufficient" to cause psychosis.[64] A French review from 2009 came to a conclusion that cannabis use, particularly that before age 15, was a factor in the development of schizophrenic disorders.[65]
Other potential long-term effects
A 2008 National Institutes of Health study of 19 chronic heavy marijuana users with cardiac and cerebral abnormalities (averaging 28 g to 272 g (1 to 9+ oz) weekly) and 24 controls found elevated levels of apolipoprotein C-III (apoC-III) in the chronic smokers.[66] An increase in apoC-III levels induces the development of hypertriglyceridemia.
Pharmacology
The genus Cannabis contains two species which produce useful amounts of psychoactive cannabinoids: Cannabis indica and Cannabis sativa, which are listed as Schedule I medicinal plants in the US;[4] a third species, Cannabis ruderalis, has few psychogenic properties.[4] Cannabis contains more than 460 compounds;[7] at least 80 of these are cannabinoids[67][68] – chemical compounds that interact with cannabinoid receptors in the brain.[4] As of 2012, more than 20 cannabinoids were being studied by the U.S. FDA.[69]
The most psychoactive cannabinoid found in the cannabis plant is tetrahydrocannabinol (or delta-9-tetrahydrocannabinol, commonly known as THC).[7] Other cannabinoids include delta-8-tetrahydrocannabinol, cannabidiol (CBD), cannabinol (CBN), cannabicyclol (CBL), cannabichromene (CBC) and cannabigerol (CBG); they have less psychotropic effects than THC, but may play a role in the overall effect of cannabis.[7] The most studied are THC, CBD and CBN.[57]
CB1 and CB2 are the primary cannabinoid receptors responsible for several of the effects of cannabinoids, although other receptors may play a role as well. Both belong to a group of receptors called G protein-coupled receptors (GPCRs). CB1 receptors are found in very high levels in the brain and are thought to be responsible for psychoactive effects.[70] CB2 receptors are found peripherally throughout the body and are thought to modulate pain and inflammation.[71]
Absorption
Cannabinoid absorption is dependent on its route of administration.
Inhaled and vaporized THC have similar absorption profiles to smoked THC, with a bioavailability ranging from 10 to 35%. Oral administration has the lowest bioavailability of approximately 6%, variable absorption depending on the vehicle used, and the longest time to peak plasma levels (2 to 6 hours) compared to smoked or vaporized THC.[72]
Similar to THC, CBD has poor oral bioavailability, approximately 6%. The low bioavailability is largely attributed to significant first-pass metabolism in the liver and erratic absorption from the gastrointestinal tract. However, oral administration of CBD has a faster time to peak concentrations (2 hours) than THC.[72]
Due to the poor bioavailability of oral preparations, alternative routes of administration have been studied, including sublingual and rectal. These alternative formulations maximize bioavailability and reduce first-pass metabolism. Sublingual administration in rabbits yielded bioavailability of 16% and time to peak concentration of 4 hours.[73] Rectal administration in monkeys doubled bioavailability to 13.5% and achieved peak blood concentrations within 1 to 8 hours after administration.[74]
Distribution
Like cannabinoid absorption, distribution is also dependent on route of administration. Smoking and inhalation of vaporized cannabis have better absorption than do other routes of administration, and therefore also have more predictable distribution.[74][75] THC is highly protein bound once absorbed, with only 3% found unbound in the plasma. It distributes rapidly to highly vascularized organs such as the heart, lungs, liver, spleen, and kidneys, as well as to various glands. Low levels can be detected in the brain, testes, and unborn fetuses, all of which are protected from systemic circulation via barriers.[76] THC further distributes into fatty tissues a few days after administration due to its high lipophilicity, and is found deposited in the spleen and fat after redistribution.[75][77][78]
Metabolism
Delta-9-THC is the primary molecule responsible for the effects of cannabis. Delta-9-THC is metabolized in the liver and turns into 11-OH-THC.[79] 11-OH-THC is the first metabolic product in this pathway. Both Delta-9-THC and 11-OH-THC are psychoactive. The metabolism of THC into 11-OH-THC plays a part in the heightened psychoactive effects of edible cannabis.[80]
Next, 11-OH-THC is metabolized in the liver into 11-COOH-THC, which is the second metabolic product of THC.[81] 11-COOH-THC is not psychoactive.[79]
Ingestion of edible cannabis products lead to a slower onset of effect than the inhalation of it because the THC travels to the liver first through the blood before it travels to the rest of the body. Inhaled cannabis can result in THC going directly to the brain, where it then travels from the brain back to the liver in recirculation for metabolism.[79] Eventually, both routes of metabolism result in the metabolism of psychoactive THC to inactive 11-COOH-THC.
Excretion
Due to substantial metabolism of THC and CBD, their metabolites are excreted mostly via feces, rather than by urine.[72][82] After delta-9-THC is hydroxylated into 11-OH-THC via CYP2C9, CYP2C19, and CYP3A4, it undergoes phase II metabolism into more than 30 metabolites, a majority of which are products of glucuronidation. Approximately 65% of THC is excreted in feces and 25% in the urine, while the remaining 10% is excreted by other means.[72] The terminal half-life of THC is 25 to 36 hours,[83] whereas for CBD it is 18 to 32 hours.[82]
CBD is hydroxylated by P450 liver enzymes into 7-OH-CBD. Its metabolites are products of primarily CYP2C19 and CYP3A4 activity, with potential activity of CYP1A1, CYP1A2, CYP2C9, and CYP2D6.[84] Similar to delta-9-THC, a majority of CBD is excreted in feces and some in the urine.[72] The terminal half-life is approximately 18–32 hours.[85]
Administration

Smoking has been the means of administration of cannabis for many users, but it is not suitable for the use of cannabis as a medicine.[86] It was the most common method of medical cannabis consumption in the US as of 2013.[4] It is difficult to predict the pharmacological response to cannabis because concentration of cannabinoids varies widely, as there are different ways of preparing it for consumption (smoked, applied as oils, eaten, infused into other foods, or drunk) and a lack of production controls.[4] The potential for adverse effects from smoke inhalation makes smoking a less viable option than oral preparations.[86] Cannabis vaporizers have gained popularity because of a perception among users that fewer harmful chemicals are ingested when components are inhaled via aerosol rather than smoke.[4] Cannabinoid medicines are available in pill form (dronabinol and nabilone) and liquid extracts formulated into an oromucosal spray (nabiximols).[4] Oral preparations are "problematic due to the uptake of cannabinoids into fatty tissue, from which they are released slowly, and the significant first-pass liver metabolism, which breaks down Δ9THC and contributes further to the variability of plasma concentrations".[86]
The US Food and Drug Administration (FDA) has not approved smoked cannabis for any condition or disease, as it deems that evidence is lacking concerning safety and efficacy.[87] The FDA issued a 2006 advisory against smoked medical cannabis stating: "marijuana has a high potential for abuse, has no currently accepted medical use in treatment in the United States, and has a lack of accepted safety for use under medical supervision."[87]
History
Ancient
Cannabis, called má 麻 (meaning "hemp; cannabis; numbness") or dàmá 大麻 (with "big; great") in Chinese, was used in Taiwan for fiber starting about 10,000 years ago.[88] The botanist Hui-lin Li wrote that in China, "The use of Cannabis in medicine was probably a very early development. Since ancient humans used hemp seed as food, it was quite natural for them to also discover the medicinal properties of the plant."[89] Emperor Shen-Nung, who was also a pharmacologist, wrote a book on treatment methods in 2737 BCE that included the medical benefits of cannabis. He recommended the substance for many ailments, including constipation, gout, rheumatism, and absent-mindedness.[90] Cannabis is one of the 50 "fundamental" herbs in traditional Chinese medicine.[91]
The Ebers Papyrus (c. 1550 BCE) from Ancient Egypt describes medical cannabis.[92] The ancient Egyptians used hemp (cannabis) in suppositories for relieving the pain of hemorrhoids.[93]
Surviving texts from ancient India confirm that cannabis' psychoactive properties were recognized, and doctors used it for treating a variety of illnesses and ailments, including insomnia, headaches, gastrointestinal disorders, and pain, including during childbirth.[94]
The Ancient Greeks used cannabis to dress wounds and sores on their horses,[95] and in humans, dried leaves of cannabis were used to treat nose bleeds, and cannabis seeds were used to expel tapeworms.[95]
In the medieval Islamic world, Arabic physicians made use of the diuretic, antiemetic, antiepileptic, anti-inflammatory, analgesic and antipyretic properties of Cannabis sativa, and used it extensively as medication from the 8th to 18th centuries.[96]
Landrace strains

Cannabis seeds may have been used for food, rituals or religious practices in ancient Europe and China.[97]:19–22 Harvesting the plant led to the spread of cannabis throughout Eurasia about 10,000 to 5,000 years ago, with further distribution to the Middle East and Africa about 2,000 to 500 years ago.[97]:18–19 A landrace strain of cannabis developed over centuries.[98] They are cultivars of the plant that originated in one specific region.
Widely cultivated strains of cannabis, such as "Afghani" or "Hindu Kush", are indigenous to the Pakistan and Afghanistan regions, while "Durban Poison" is native to Africa.[97]:45–48 There are approximately 16 landrace strains of cannabis identified from Pakistan, Jamaica, Africa, Mexico, Central America and Asia.[99]
Modern
An Irish physician, William Brooke O'Shaughnessy, is credited with introducing cannabis to Western medicine.[100] O'Shaughnessy discovered cannabis in the 1830s while living abroad in India, where he conducted numerous experiments investigating the drug's medical utility (noting in particular its analgesic and anticonvulsant effects).[101] He returned to England with a supply of cannabis in 1842, after which its use spread through Europe and the United States.[102] In 1845 French physician Jacques-Joseph Moreau published a book about the use of cannabis in psychiatry.[103] In 1850 cannabis was entered into the United States Pharmacopeia.[101]
The use of cannabis in medicine began to decline by the end of the 19th century, due to difficulty in controlling dosages and the rise in popularity of synthetic and opium-derived drugs.[102] Also, the advent of the hypodermic syringe allowed these drugs to be injected for immediate effect, in contrast to cannabis which is not water-soluble and therefore cannot be injected.[102]
In the United States, the medical use of cannabis further declined with the passage of the Marihuana Tax Act of 1937, which imposed new regulations and fees on physicians prescribing cannabis.[104] Cannabis was removed from the U.S. Pharmacopeia in 1941, and officially banned for any use with the passage of the Controlled Substances Act of 1970.[102]
Cannabis began to attract renewed interest as medicine in the 1970s and 1980s, in particular due to its use by cancer and AIDS patients who reported relief from the effects of chemotherapy and wasting syndrome.[105] In 1996, California became the first U.S. state to legalize medical cannabis in defiance of federal law.[106] In 2001, Canada became the first country to adopt a system regulating the medical use of cannabis.[107]
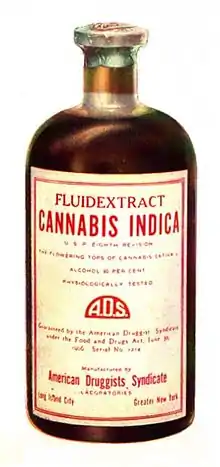 Cannabis indica fluid extract, American Druggists Syndicate, pre-1937
Cannabis indica fluid extract, American Druggists Syndicate, pre-1937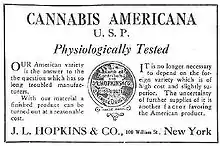 An advertisement for cannabis americana distributed by a pharmacist in New York in 1917
An advertisement for cannabis americana distributed by a pharmacist in New York in 1917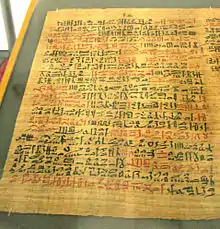 The Ebers Papyrus (c. 1550 BCE) from Ancient Egypt has a prescription for medical marijuana applied directly for inflammation.
The Ebers Papyrus (c. 1550 BCE) from Ancient Egypt has a prescription for medical marijuana applied directly for inflammation.
Society and culture
Legal status

See also countries that have decriminalized or where enforcement is limited.
Countries that have legalized the medical use of cannabis include Australia,[108] Brazil,[109] Canada,[110] Chile,[110] Colombia,[110] Croatia,[111] Cyprus,[112] Czech Republic,[110] Finland,[113] Germany,[114] Greece,[115] Israel,[116] Italy,[117] Jamaica,[118] Lebanon,[119] Luxembourg,[120] North Macedonia,[121] Malta,[122] the Netherlands,[110] New Zealand,[123] Peru,[124] Poland,[125] Portugal,[126] Sri Lanka,[127] Thailand,[128] the United Kingdom,[129] and Uruguay.[110] Other countries have more restrictive laws that allow only the use of isolated cannabinoid drugs such as Sativex or Epidiolex.[130][131] Countries with the most relaxed policies include Canada,[132] Uruguay,[110] and the Netherlands,[110] where cannabis can be purchased without need for a prescription. In Mexico, THC content of medical cannabis is limited to one percent.[133] The same limit applies in Switzerland, but no prescription is required to purchase.[134] In the United States, the legality of medical cannabis varies by state.[11]
Cannabis and its derivatives are subject to regulation under three United Nations treaties: the 1961 Single Convention on Narcotic Drugs, the 1971 Convention on Psychotropic Substances, and the 1988 Convention Against Illicit Traffic in Narcotic Drugs and Psychotropic Substances.[135] Cannabis is classified as a Schedule I drug under the Single Convention treaty, meaning that medical use is allowed but that it is considered to be an addictive drug with a serious risk of abuse – along with other drugs such as opium and cocaine.[136] Prior to December 2020 it was also included in Schedule IV, a subset of Schedule I, which is for only the most dangerous drugs such as heroin and fentanyl.[137] Member nations of the UN Commission on Narcotic Drugs voted 27–25 to remove it from Schedule IV on December 2, 2020,[138] following a World Health Organization recommendation for removal in January 2019.[139][140]
United States
In the United States, the use of cannabis for medical purposes is legal in 35 states, four out of five permanently inhabited U.S. territories, and the District of Columbia.[11] An additional 13 states have more restrictive laws allowing the use of low-THC products.[11] Cannabis remains illegal at the federal level under the Controlled Substances Act, which classifies it as a Schedule I drug with a high potential for abuse and no accepted medical use. In December 2014, however, the Rohrabacher–Farr amendment was signed into law, prohibiting the Justice Department from prosecuting individuals acting in accordance with state medical cannabis laws.[141]
Distribution

The method of obtaining medical cannabis varies by region and by legislation. In the US, most consumers grow their own or buy it from cannabis dispensaries in states where it is legal.[4][142] Marijuana vending machines for selling or dispensing cannabis are in use in the United States and are planned to be used in Canada.[143] In 2014, the startup Meadow began offering on-demand delivery of medical marijuana in the San Francisco Bay Area, through their mobile app.[144]
Almost 70% of medical cannabis is exported from the United Kingdom, according to a 2017 United Nations report, with much of the remaining amount coming from Canada and the Netherlands.[145]
Insurance
In the United States, health insurance companies may not pay for a medical marijuana prescription as the Food and Drug Administration must approve any substance for medicinal purposes. Before this can happen, the FDA must first permit the study of the medical benefits and drawbacks of the substance, which it has not done since it was placed on Schedule I of the Controlled Substances Act in 1970. Therefore, all expenses incurred fulfilling a medical marijuana prescription will possibly be incurred as out-of-pocket.[146] However, the New Mexico Court of Appeals has ruled that workers' compensation insurance must pay for prescribed marijuana as part of the state's Medical Cannabis Program.[147]
Positions of medical organizations
Medical organizations that have issued statements in support of allowing access to medical cannabis include the American Nurses Association,[8] American Public Health Association,[148] American Medical Student Association,[149] National Multiple Sclerosis Society,[150] Epilepsy Foundation,[151] and Leukemia & Lymphoma Society.[152]
Organizations that oppose the legalization of medical cannabis include the American Academy of Pediatrics[10] and American Psychiatric Association.[153] However, the AAP also supports rescheduling for the purpose of facilitating research.[10]
The American Medical Association[154] and American College of Physicians[155] do not take a position on the legalization of medical cannabis, but have called for the Schedule I classification to be reviewed. The American Academy of Family Physicians[9] and American Society of Addiction Medicine[156] also do not take a position, but do support rescheduling to better facilitate research. The American Heart Association says that "many of the concerning health implications of cannabis include cardiovascular diseases" but that it supports rescheduling to allow "more nuanced ... marijuana legislation and regulation" and to "reflect the existing science behind cannabis".[157] The American Cancer Society[158] and American Psychological Association[159] have noted the obstacles that exist for conducting research on cannabis, and have called on the federal government to better enable scientific study of the drug.
Cancer Research UK say that while cannabis is being studied for therapeutic potential, "claims that there is solid 'proof' that cannabis or cannabinoids can cure cancer is highly misleading to patients and their families, and builds a false picture of the state of progress in this area".[160]
Recreational use
The authors of a report on a 2011 survey of medical cannabis users say that critics have suggested that some users "game the system" to obtain medical cannabis ostensibly for treatment of a condition, but then use it for nonmedical purposes – though the truth of this claim is hard to measure.[161] The report authors suggested rather that medical cannabis users occupied a "continuum" between medical and nonmedical use.[161]
Brand names
In the US, the FDA has approved two oral cannabinoids for use as medicine: dronabinol and nabilone.[4] Dronabinol, synthetic THC, is listed as Schedule II.[162] Nabilone, a synthetic cannabinoid, is also Schedule II, indicating high potential for side effects and addiction.[69] Both received approval for sale in the US in 1985, under the brand names Marinol and Cesamet.[163] Nabiximols, an oromucosal spray derived from two strains of Cannabis sativa and containing THC and CBD,[69] is not approved in the United States, but is approved in several European countries, Canada, and New Zealand as of 2013.[4] As of 2018, medical marijuana in Canada is being legally distributed to registered patients in bud, drops and capsule forms by such companies as Canopy Growth Corp. and Aurora Cannabis.
| Generic medication |
Brand name(s) |
Country | Licensed indications |
|---|---|---|---|
| Nabilone | Cesamet | U.S., Canada | Antiemetic (treatment of nausea or vomiting) associated with chemotherapy that has failed to respond adequately to conventional therapy[4] |
| Dronabinol | Marinol | ||
| Syndros | U.S. | Anorexia associated with AIDS–related weight loss[4] | |
| Nabiximols | Sativex | Canada, New Zealand, majority of the EU[164] |
Limited treatment for spasticity and neuropathic pain associated with multiple sclerosis and intractable cancer pain.[4] |
As an antiemetic, these medications are usually used when conventional treatment for nausea and vomiting associated with cancer chemotherapy fail to work.[4]
Nabiximols is used for treatment of spasticity associated with MS when other therapies have not worked, and when an initial trial demonstrates "meaningful improvement".[4] Trials for FDA approval in the US are underway.[4] It is also approved in several European countries for overactive bladder and vomiting.[69] When sold under the trade name Sativex as a mouth spray, the prescribed daily dose in Sweden delivers a maximum of 32.4 mg of THC and 30 mg of CBD; mild to moderate dizziness is common during the first few weeks.[165]
Relative to inhaled consumption, peak concentration of oral THC is delayed, and it may be difficult to determine optimal dosage because of variability in patient absorption.[4]
In 1964, Albert Lockhart and Manley West began studying the health effects of traditional cannabis use in Jamaican communities. They developed, and in 1987 gained permission to market, the pharmaceutical "Canasol", one of the first cannabis extracts.[166]
Research
Medical cannabis research includes any medical research on using cannabis as a treatment for any medical condition. For reasons including increased popular support of cannabis use, a trend of cannabis legalization, and the perception of medical usefulness, more scientists are doing medical cannabis research. Medical cannabis is unusually broad as a treatment for many conditions, each of which has its own state of research. Similarly, various countries conduct and respond to medical cannabis research in different ways.
References
- Murnion B (December 2015). "Medicinal cannabis". Australian Prescriber. 38 (6): 212–5. doi:10.18773/austprescr.2015.072. PMC 4674028. PMID 26843715.
- "What is medical marijuana?". National Institute of Drug Abuse. July 2015. Retrieved 19 April 2016.
The term medical marijuana refers to using the whole unprocessed marijuana plant or its basic extracts to treat a disease or symptom.
- "Release the strains". Nature Medicine. 21 (9): 963. September 2015. doi:10.1038/nm.3946. PMID 26340110.
- Borgelt LM, Franson KL, Nussbaum AM, Wang GS (February 2013). "The pharmacologic and clinical effects of medical cannabis" (PDF). Pharmacotherapy. 33 (2): 195–209. doi:10.1002/phar.1187. PMID 23386598. S2CID 8503107.
- Whiting PF, Wolff RF, Deshpande S, Di Nisio M, Duffy S, Hernandez AV, Keurentjes JC, Lang S, Misso K, Ryder S, Schmidlkofer S, Westwood M, Kleijnen J (23 June 2015). "Cannabinoids for Medical Use: A Systematic Review and Meta-analysis". JAMA. 313 (24): 2456–73. doi:10.1001/jama.2015.6358. PMID 26103030.
- Jensen B, Chen J, Furnish T, Wallace M (October 2015). "Medical Marijuana and Chronic Pain: a Review of Basic Science and Clinical Evidence". Current Pain and Headache Reports. 19 (10): 50. doi:10.1007/s11916-015-0524-x. PMID 26325482. S2CID 9110606.
- Ben Amar M (April 2006). "Cannabinoids in medicine: A review of their therapeutic potential". Journal of Ethnopharmacology (Review). 105 (1–2): 1–25. CiteSeerX 10.1.1.180.308. doi:10.1016/j.jep.2006.02.001. PMID 16540272.
- Therapeutic Use of Marijuana and Related Cannabinoids (PDF), American Nurses Association, 2016
- "AAFP Releases Marijuana, Cannabinoids Position Paper". American Academy of Family Physicians. 20 September 2019. Retrieved 6 October 2019.
- American Academy of Pediatrics Reaffirms Opposition to Legalizing Marijuana for Recreational or Medical Use, American Academy of Pediatrics, 26 January 2015, retrieved 30 July 2017
- "State Medical Marijuana Laws". National Conference of State Legislatures. 27 June 2018. Retrieved 3 July 2018.
- "Marijuana as Medicine". National Institute on Drug Abuse. July 2019.
- Consumer Reports (28 April 2016). "Up in Smoke: Does Medical Marijuana Work?". Consumer Reports. Retrieved 24 May 2016.
- Schubart CD, Sommer IE, Fusar-Poli P, de Witte L, Kahn RS, Boks MP (January 2014). "Cannabidiol as a potential treatment for psychosis" (PDF). European Neuropsychopharmacology. 24 (1): 51–64. doi:10.1016/j.euroneuro.2013.11.002. PMID 24309088. S2CID 13197304.
- Koppel BS, Brust JC, Fife T, Bronstein J, Youssof S, Gronseth G, Gloss D (April 2014). "Systematic review: efficacy and safety of medical marijuana in selected neurologic disorders: report of the Guideline Development Subcommittee of the American Academy of Neurology". Neurology. 82 (17): 1556–63. doi:10.1212/WNL.0000000000000363. PMC 4011465. PMID 24778283.
- Pratt M, Stevens A, Thuku M, Butler C, Skidmore B, Wieland LS, Clemons M, Kanji S, Hutton B (December 2019). "Benefits and harms of medical cannabis: a scoping review of systematic reviews". Syst Rev (Systematic review). 8 (1): 320. doi:10.1186/s13643-019-1243-x. PMC 6905063. PMID 31823819.
- Sachs J, McGlade E, Yurgelun-Todd D (October 2015). "Safety and Toxicology of Cannabinoids". Neurotherapeutics. 12 (4): 735–46. doi:10.1007/s13311-015-0380-8. PMC 4604177. PMID 26269228.
- "Sex(ism), Drugs, and Migraines: Distillations Podcast and Transcript, Episode 237". Distillations. Science History Institute. 15 January 2019. Retrieved 28 August 2019.
- Gilson, Aaron M.; LeBaron, Virginia T.; Vyas, Marianne Beare (1 January 2018). "The use of cannabis in response to the opioid crisis: A review of the literature". Nursing Outlook. 66 (1): 56–65. doi:10.1016/j.outlook.2017.08.012. ISSN 0029-6554. PMID 28993073.
- American College of Obstetricians Gynecologists Committee on Obstetric Practice (July 2015). "Committee Opinion No. 637: Marijuana Use During Pregnancy and Lactation". Obstetrics and Gynecology. 126 (1): 234–8. doi:10.1097/01.AOG.0000467192.89321.a6. PMID 26241291.
- Grotenhermen F, Müller-Vahl K (July 2012). "The therapeutic potential of cannabis and cannabinoids". Deutsches Ärzteblatt International. 109 (29–30): 495–501. doi:10.3238/arztebl.2012.0495. PMC 3442177. PMID 23008748.
- Bowles DW, O'Bryant CL, Camidge DR, Jimeno A (July 2012). "The intersection between cannabis and cancer in the United States". Critical Reviews in Oncology/Hematology (Review). 83 (1): 1–10. doi:10.1016/j.critrevonc.2011.09.008. PMID 22019199.
- Wang T, Collet JP, Shapiro S, Ware MA (June 2008). "Adverse effects of medical cannabinoids: a systematic review". CMAJ (Review). 178 (13): 1669–78. doi:10.1503/cmaj.071178. PMC 2413308. PMID 18559804.
- Jordan K, Sippel C, Schmoll HJ (September 2007). "Guidelines for antiemetic treatment of chemotherapy-induced nausea and vomiting: past, present, and future recommendations" (PDF). The Oncologist (Review). 12 (9): 1143–50. doi:10.1634/theoncologist.12-9-1143. PMID 17914084. S2CID 17612434.
- Nicolson SE, Denysenko L, Mulcare JL, Vito JP, Chabon B (May–June 2012). "Cannabinoid hyperemesis syndrome: a case series and review of previous reports". Psychosomatics (Review, case series). 53 (3): 212–9. doi:10.1016/j.psym.2012.01.003. PMID 22480624.
- Phillips RS, Friend AJ, Gibson F, Houghton E, Gopaul S, Craig JV, Pizer B (February 2016). "Antiemetic medication for prevention and treatment of chemotherapy-induced nausea and vomiting in childhood" (PDF). The Cochrane Database of Systematic Reviews. 2: CD007786. doi:10.1002/14651858.CD007786.pub3. PMC 7073407. PMID 26836199.
- Lutge EE, Gray A, Siegfried N (April 2013). "The medical use of cannabis for reducing morbidity and mortality in patients with HIV/AIDS". The Cochrane Database of Systematic Reviews (Review). 4 (4): CD005175. doi:10.1002/14651858.CD005175.pub3. PMID 23633327.
- Aviram J, Samuelly-Leichtag G (September 2017). "Efficacy of Cannabis-Based Medicines for Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled Trials". Pain Physician. 20 (6): E755–E796. PMID 28934780.
- Lynch ME, Campbell F (November 2011). "Cannabinoids for treatment of chronic non-cancer pain; a systematic review of randomized trials". British Journal of Clinical Pharmacology (Review). 72 (5): 735–44. doi:10.1111/j.1365-2125.2011.03970.x. PMC 3243008. PMID 21426373.
- Carter GT, Flanagan AM, Earleywine M, Abrams DI, Aggarwal SK, Grinspoon L (August 2011). "Cannabis in palliative medicine: improving care and reducing opioid-related morbidity". The American Journal of Hospice & Palliative Care (Review). 28 (5): 297–303. doi:10.1177/1049909111402318. PMID 21444324. S2CID 19980960.
- Clark PA, Capuzzi K, Fick C (December 2011). "Medical marijuana: medical necessity versus political agenda". Medical Science Monitor (Review). 17 (12): RA249–61. doi:10.12659/MSM.882116. PMC 3628147. PMID 22129912.
- Oreja-Guevara C (October 2012). "[Treatment of spasticity in multiple sclerosis: new perspectives regarding the use of cannabinoids]". Revista de Neurología (Review) (in Spanish). 55 (7): 421–30. PMID 23011861.
- Commissioner, Office of the (10 June 2019). "FDA and Marijuana". FDA.
- Black N, Stockings E, Campbell G, Tran LT, Zagic D, Hall WD, Farrell M, Degenhardt L (December 2019). "Cannabinoids for the treatment of mental disorders and symptoms of mental disorders: a systematic review and meta-analysis". Lancet Psychiatry (Systematic review & meta-analysis). 6 (12): 995–1010. doi:10.1016/S2215-0366(19)30401-8. PMC 6949116. PMID 31672337.
- Washington TA, Brown KM, Fanciullo GJ (2012). "Chapter 31: Medical Cannabis". Pain. Oxford University Press. p. 165. ISBN 978-0-19-994274-9.
Proponents of medical cannabis site its safety, but there studies in later years that support that smoking of marijuana is associated with risk for dependence and that THC alters the structures of cells in the brain
- Gage SH, Hickman M, Zammit S (April 2016). "Association Between Cannabis and Psychosis: Epidemiologic Evidence". Biological Psychiatry. 79 (7): 549–56. doi:10.1016/j.biopsych.2015.08.001. hdl:1983/b8fb2d3b-5a55-4d07-97c0-1650b0ffc05d. PMID 26386480. S2CID 1055335.
- Barceloux, Donald G (2012). "Chapter 60: Marijuana (Cannabis sativa L.) and synthetic cannabinoids". Medical Toxicology of Drug Abuse: Synthesized Chemicals and Psychoactive Plants. pp. 886–931. ISBN 978-0-471-72760-6.
- Hall W, Solowij N (November 1998). "Adverse effects of cannabis". Lancet. 352 (9140): 1611–6. doi:10.1016/S0140-6736(98)05021-1. PMID 9843121. S2CID 16313727.
- "Sativex Oral Mucosal Spray Public Assessment Report. Decentralized Procedure" (PDF). United Kingdom Medicines and Healthcare Products Regulatory Agency. p. 93. Retrieved 7 May 2015.
There is clear evidence that recreational cannabis can produce a transient toxic psychosis in larger doses or in susceptible individuals, which is said to characteristically resolve within a week or so of absence (Johns 2001). Transient psychotic episodes as a component of acute intoxication are well-documented (Hall et al 1994)
- D'Souza DC, Sewell RA, Ranganathan M (October 2009). "Cannabis and psychosis/schizophrenia: human studies". European Archives of Psychiatry and Clinical Neuroscience. 259 (7): 413–31. doi:10.1007/s00406-009-0024-2. PMC 2864503. PMID 19609589.
- "Drug Abuse Warning Network, 2011. National Estimates of Drug-Related Emergency Department Visits" (PDF). U.S. Department of Health and Human Services. 2011. Retrieved 8 May 2015.
- "www.samhsa.gov".
- Volkow ND, Baler RD, Compton WM, Weiss SR (June 2014). "Adverse health effects of marijuana use". The New England Journal of Medicine. 370 (23): 2219–27. doi:10.1056/NEJMra1402309. PMC 4827335. PMID 24897085.
- Hall W (January 2015). "What has research over the past two decades revealed about the adverse health effects of recreational cannabis use?" (PDF). Addiction. 110 (1): 19–35. doi:10.1111/add.12703. PMID 25287883.
- Zehra, Amna; Burns, Jamie; Liu, Christopher Kure; Manza, Peter; Wiers, Corinde E.; Volkow, Nora D.; Wang, Gene-Jack (2018). "Cannabis Addiction and the Brain: a Review". Journal of Neuroimmune Pharmacology. 13 (4): 438–452. doi:10.1007/s11481-018-9782-9. ISSN 1557-1890. PMC 6223748. PMID 29556883.
- Maisto S, Galizio M, Connors G (2014). Drug Use and Abuse. Cengage Learning. p. 278. ISBN 978-1-305-17759-8.
- Tashkin DP (June 2013). "Effects of marijuana smoking on the lung" (PDF). Annals of the American Thoracic Society. 10 (3): 239–47. doi:10.1513/annalsats.201212-127fr. PMID 23802821. S2CID 20615545.
- Hashibe M, Straif K, Tashkin DP, Morgenstern H, Greenland S, Zhang ZF (April 2005). "Epidemiologic review of marijuana use and cancer risk". Alcohol. 35 (3): 265–75. doi:10.1016/j.alcohol.2005.04.008. PMID 16054989.
- "Does smoking cannabis cause cancer?". Cancer Research UK. 20 September 2010. Archived from the original on 29 July 2012. Retrieved 9 January 2013. Cite journal requires
|journal=(help) - Tashkin, Donald (March 1997). "Effects of marijuana on the lung and its immune defenses". UCLA School of Medicine. Retrieved 23 June 2012. Cite journal requires
|journal=(help) - A. Riecher-Rössler (2014). Comorbidity of Mental and Physical Disorders. Karger Medical and Scientific Publishers. p. 88. ISBN 978-3-318-02604-7.
- Cottencin O, Karila L, Lambert M, Arveiller C, Benyamina A, Boissonas A, Goudemand M, Reynaud M (December 2010). "Cannabis arteritis: review of the literature". Journal of Addiction Medicine. 4 (4): 191–6. doi:10.1097/ADM.0b013e3181beb022. PMID 21769037. S2CID 33364433.
- Thomas G, Kloner RA, Rezkalla S (January 2014). "Adverse cardiovascular, cerebrovascular, and peripheral vascular effects of marijuana inhalation: what cardiologists need to know". The American Journal of Cardiology. 113 (1): 187–90. doi:10.1016/j.amjcard.2013.09.042. PMID 24176069.
- Jones RT (November 2002). "Cardiovascular system effects of marijuana". Journal of Clinical Pharmacology (Review). 42 (S1): 58S–63S. doi:10.1002/j.1552-4604.2002.tb06004.x. PMID 12412837. S2CID 12193532.
- "Withdrawal Symptoms From Smoking Pot?". WebMD.
- Hall W, Degenhardt L (October 2009). "Adverse health effects of non-medical cannabis use". Lancet. 374 (9698): 1383–91. doi:10.1016/s0140-6736(09)61037-0. PMID 19837255. S2CID 31616272.
- Gordon AJ, Conley JW, Gordon JM (December 2013). "Medical consequences of marijuana use: a review of current literature". Current Psychiatry Reports (Review). 15 (12): 419. doi:10.1007/s11920-013-0419-7. PMID 24234874. S2CID 29063282.
- "Get Medical Marijuana Card Online in 10 Mins - Medical Marijuana Doctor". Get a Medical Marijuana Card Online - California Cannabis Doctors. Retrieved 5 October 2019.
- Crean RD, Crane NA, Mason BJ (March 2011). "An evidence based review of acute and long-term effects of cannabis use on executive cognitive functions". Journal of Addiction Medicine. 5 (1): 1–8. doi:10.1097/ADM.0b013e31820c23fa. PMC 3037578. PMID 21321675.
- Martín-Santos R, Fagundo AB, Crippa JA, Atakan Z, Bhattacharyya S, Allen P, Fusar-Poli P, Borgwardt S, Seal M, Busatto GF, McGuire P (March 2010). "Neuroimaging in cannabis use: a systematic review of the literature" (PDF). Psychological Medicine. 40 (3): 383–98. doi:10.1017/S0033291709990729. PMID 19627647.
- Grant I, Gonzalez R, Carey CL, Natarajan L, Wolfson T (July 2003). "Non-acute (residual) neurocognitive effects of cannabis use: a meta-analytic study" (PDF). Journal of the International Neuropsychological Society. 9 (5): 679–89. doi:10.1017/S1355617703950016. PMID 12901774. S2CID 4894703. Lay summary – WebMD (1 July 2003).
- Large M, Sharma S, Compton MT, Slade T, Nielssen O (June 2011). "Cannabis use and earlier onset of psychosis: a systematic meta-analysis". Archives of General Psychiatry. 68 (6): 555–61. doi:10.1001/archgenpsychiatry.2011.5. PMID 21300939.
- Semple DM, McIntosh AM, Lawrie SM (March 2005). "Cannabis as a risk factor for psychosis: systematic review". Journal of Psychopharmacology. 19 (2): 187–94. doi:10.1177/0269881105049040. PMID 15871146. S2CID 44651274.
- Arseneault L, Cannon M, Witton J, Murray RM (February 2004). "Causal association between cannabis and psychosis: examination of the evidence". The British Journal of Psychiatry. 184 (2): 110–7. doi:10.1192/bjp.184.2.110. PMID 14754822.
- Laqueille X (September 2009). "[Is cannabis a vulnerability factor in schizophrenic disorders]" [Is cannabis is a vulnerability factor of schizophrenic disorders?]. Archives de Pédiatrie. 16 (9): 1302–5. doi:10.1016/j.arcped.2009.03.016. PMID 19640690.
- Jayanthi S, Buie S, Moore S, Herning RI, Better W, Wilson NM, Contoreggi C, Cadet JL (January 2010). "Heavy marijuana users show increased serum apolipoprotein C-III levels: evidence from proteomic analyses". Molecular Psychiatry. 15 (1): 101–12. doi:10.1038/mp.2008.50. PMC 2797551. PMID 18475272. Lay summary – Reuters (13 May 2008).
- Downer EJ, Campbell VA (January 2010). "Phytocannabinoids, CNS cells and development: a dead issue?". Drug and Alcohol Review (Review). 29 (1): 91–8. doi:10.1111/j.1465-3362.2009.00102.x. PMID 20078688.
- Burns TL, Ineck JR (February 2006). "Cannabinoid analgesia as a potential new therapeutic option in the treatment of chronic pain". The Annals of Pharmacotherapy (Review). 40 (2): 251–60. doi:10.1345/aph.1G217. PMID 16449552. S2CID 6858360.
- Svrakic DM, Lustman PJ, Mallya A, Lynn TA, Finney R, Svrakic NM (2012). "Legalization, decriminalization & medicinal use of cannabis: a scientific and public health perspective". Missouri Medicine (Review). 109 (2): 90–8. PMC 6181739. PMID 22675784.
- Mackie K (May 2008). "Cannabinoid receptors: where they are and what they do". Journal of Neuroendocrinology. 20 Suppl 1: 10–4. doi:10.1111/j.1365-2826.2008.01671.x. PMID 18426493. S2CID 20161611.
- Whiteside GT, Lee GP, Valenzano KJ (2007). "The role of the cannabinoid CB2 receptor in pain transmission and therapeutic potential of small molecule CB2 receptor agonists". Current Medicinal Chemistry. 14 (8): 917–36. doi:10.2174/092986707780363023. PMID 17430144.
- Gaston TE, Friedman D (May 2017). "Pharmacology of cannabinoids in the treatment of epilepsy". Epilepsy & Behavior. Cannabinoids and Epilepsy. 70 (Pt B): 313–318. doi:10.1016/j.yebeh.2016.11.016. PMID 28087250. S2CID 3929024.
- Mannila J, Järvinen T, Järvinen K, Tervonen J, Jarho P (March 2006). "Sublingual administration of Delta9-tetrahydrocannabinol/beta-cyclodextrin complex increases the bioavailability of Delta9-tetrahydrocannabinol in rabbits". Life Sciences. 78 (17): 1911–4. doi:10.1016/j.lfs.2005.08.025. PMID 16266727.
- Huestis MA (August 2007). "Human cannabinoid pharmacokinetics". Chemistry & Biodiversity. 4 (8): 1770–804. doi:10.1002/cbdv.200790152. PMC 2689518. PMID 17712819.
- Badowski ME (September 2017). "A review of oral cannabinoids and medical marijuana for the treatment of chemotherapy-induced nausea and vomiting: a focus on pharmacokinetic variability and pharmacodynamics". Cancer Chemotherapy and Pharmacology. 80 (3): 441–449. doi:10.1007/s00280-017-3387-5. PMC 5573753. PMID 28780725.
- Nahas GG (April 2001). "The pharmacokinetics of THC in fat and brain: resulting functional responses to marihuana smoking". Human Psychopharmacology. 16 (3): 247–255. doi:10.1002/hup.258. PMID 12404577. S2CID 30513770.
- Bridgeman MB, Abazia DT (March 2017). "Medicinal Cannabis: History, Pharmacology, And Implications for the Acute Care Setting". P & T. 42 (3): 180–188. PMC 5312634. PMID 28250701.
- Nahas GG, Sutin KM, Harvey DJ, Agurell S (5 April 1999). Marihuana and Medicine. Springer Science & Business Media. ISBN 978-1-59259-710-9.
- "Human Metabolism of THC". Sapiensoup Blog. 21 December 2016. Retrieved 1 November 2017.
- "11-Hydroxy-THC - Increased Potency That Explains the Effect of Edibles? - Prof of Pot". profofpot.com. Retrieved 1 November 2017.
- "Toxicology Litigation Support: Marijuana". consultox.com. Retrieved 1 November 2017.
- Devinsky O, Cilio MR, Cross H, Fernandez-Ruiz J, French J, Hill C, Katz R, Di Marzo V, Jutras-Aswad D, Notcutt WG, Martinez-Orgado J, Robson PJ, Rohrback BG, Thiele E, Whalley B, Friedman D (June 2014). "Cannabidiol: pharmacology and potential therapeutic role in epilepsy and other neuropsychiatric disorders". Epilepsia. 55 (6): 791–802. doi:10.1111/epi.12631. PMC 4707667. PMID 24854329.
- Grotenhermen F (1 April 2003). "Pharmacokinetics and pharmacodynamics of cannabinoids". Clinical Pharmacokinetics. 42 (4): 327–60. doi:10.2165/00003088-200342040-00003. PMID 12648025. S2CID 25623600.
- Juřica, Ondřej Zendulka, Gabriela Dovrtělová, Kristýna Nosková, Miroslav Turjap, Alexandra Šulcová, Lumír Hanuš and Jan (29 February 2016). "Cannabinoids and Cytochrome P450 Interactions". Current Drug Metabolism. 17 (3).
- Ohlsson A, Lindgren JE, Andersson S, Agurell S, Gillespie H, Hollister LE (February 1986). "Single-dose kinetics of deuterium-labelled cannabidiol in man after smoking and intravenous administration". Biomedical & Environmental Mass Spectrometry. 13 (2): 77–83. doi:10.1002/bms.1200130206. PMID 2937482.
- Curtis A, Clarke CE, Rickards HE (October 2009). "Cannabinoids for Tourette's Syndrome". The Cochrane Database of Systematic Reviews (Review) (4): CD006565. doi:10.1002/14651858.CD006565.pub2. PMC 7387115. PMID 19821373.
- "Inter-agency advisory regarding claims that smoked marijuana is a medicine" (Press release). fda.gov. 20 April 2006. Retrieved 24 December 2012.
- Abel, Ernest L. (1980). "Cannabis in the Ancient World". Marihuana: the first twelve thousand years. New York City: Plenum Publishers. ISBN 978-0-306-40496-2.
- Li, Hui-Lin (1974). "An Archaeological and Historical Account of Cannabis in China", Economic Botany 28.4:437–448, p. 444.
- Bloomquist, Edward (1971). Marijuana: The Second Trip. California: Glencoe Press.
- Wong, Ming (1976). La Médecine chinoise par les plantes. Paris: Tchou. OCLC 2646789.
- "The Ebers Papyrus The Oldest (confirmed) Written Prescriptions For Medical Marihuana era 1,550 BC". onlinepot.org. Retrieved 10 June 2008.
- Pain, Stephanie (15 December 2007). "The Pharaoh's pharmacists". New Scientist. Reed Business Information Ltd.
- Touw M (1981). "The religious and medicinal uses of Cannabis in China, India and Tibet". Journal of Psychoactive Drugs. 13 (1): 23–34. doi:10.1080/02791072.1981.10471447. PMID 7024492.
- Butrica, James L. (2002). "The Medical Use of Cannabis Among the Greeks and Romans" (PDF). Journal of Cannabis Therapeutics. 2 (2): 51–70. doi:10.1300/J175v02n02_04. Retrieved 8 November 2014.
- Lozano, Indalecio (2001). "The Therapeutic Use of Cannabis sativa (L.) in Arabic Medicine". Journal of Cannabis Therapeutics. 1: 63–70. CiteSeerX 10.1.1.550.1717. doi:10.1300/J175v01n01_05.
- Holland, Julie (Editor) (2010). The Pot Book: A Complete Guide to Cannabis. New York: Simon and Schuster. ISBN 978-1594778988. Retrieved 22 April 2018.CS1 maint: extra text: authors list (link)
- Evert RF, Eichhorn SE (2013). Raven Biology of Plants (8th ed.). New York, NY: W. H. Freeman and Company. pp. 213–217. ISBN 978-1-4292-1961-7.
- Evert RF, Eichhorn SE (2013). Raven Biology of Plants (8th ed.). New York, NY: W.H. Freeman and Company. pp. 501–504. ISBN 9781429219617.
- Alison Mack; Janet Joy (7 December 2000). Marijuana As Medicine?: The Science Beyond the Controversy. National Academies Press. pp. 15–. ISBN 978-0-309-06531-3.
- Booth, Martin (June 2005). Cannabis: A History. New York: St. Martin's Press. ISBN 978-0-312-42494-7.
- Grinspoon L, Bakalar J (1997). Marihuana, the Forbidden Medicine (Revised and expanded ed.). Yale University Press. ISBN 978-0-300-07086-6.
- Hans Bangen:Geschichte der medikamentösen Therapie der Schizophrenie. Berlin 1992, Page 22.
- Pacula, Rosalie Piccardo (February 2002). "State Medical Marijuana Laws: Understanding the Laws and Their Limitations" (PDF). Journal of Public Health Policy. 23 (4): 413–439. CiteSeerX 10.1.1.202.2274. doi:10.2307/3343240. JSTOR 3343240. PMID 12532682. S2CID 13389317.
- Joy JE, Watson SJ, Benson JA (1999). "Marijuana and Medicine -- Assessing the Science Base" (PDF). Washington, D.C.: National Academy Press. Archived from the original (PDF) on 23 January 2018. Retrieved 28 July 2017.
- "History of Marijuana as Medicine – 2900 BC to Present". ProCon.org. Retrieved 27 July 2017.
- "Marijuana's journey to legal health treatment: the Canadian experience". CBC News. 17 August 2009. Retrieved 27 July 2017.
- Jolly, William (28 February 2018). "Medicinal Marijuana Legal In Australia". Canstar. Retrieved 16 July 2018.
- Ponieman, Natan (3 December 2019). "Brazil Regulates Sale Of Medical Marijuana Products". Benzinga. Retrieved 10 December 2019.
- Williams, Sean (15 May 2016). "10 Countries (Aside From the U.S.) Where Some Form of Medical Marijuana Is Legal". The Motley Fool. Retrieved 5 November 2017.
- Veselica, Lajla (15 October 2015). "Croatia legalises marijuana for medical use". Yahoo News. AFP. Retrieved 4 November 2017.
- "Cyprus begins to distribute medical cannabis". InCyprus. 22 May 2017. Archived from the original on 9 June 2017. Retrieved 11 November 2017.
- "Legal status of cannabis in Finland – An overview". Sensi Seeds. Retrieved 4 November 2017.
- Senthilingam, Meera (6 March 2017). "Germany joins the global experiment on marijuana legalization". CNN.com. Retrieved 4 November 2017.
- Revesz, Rachael (3 July 2017). "Greece legalises marijuana for medical purposes". The Independent. Retrieved 4 November 2017.
- Schwartz, Yardena (24 August 2017). "How the Booming Israeli Weed Industry Is Changing American Pot". Rollingstone.com. Retrieved 4 November 2017.
- Samuels, Gabriel (26 July 2016). "Italian army aims to produce 'the best-quality' medical marijuana after finding current batches deficient". The Independent. Retrieved 4 November 2017.
- Bud, Monterey (19 March 2018). "Jamaica's Kaya Farms Becomes First Medical Marijuana Dispensary To Open". marijuana.com. Retrieved 16 July 2018.
- "Lebanon Legalizes Cannabis Farming for Medicinal Use". The New York Times. Reuters. 21 April 2020.
- Pritchard, Heledd (29 June 2018). "Cannabis for medical use legalised in Luxembourg". Luxembourg Times. Retrieved 8 July 2018.
- Marusic, Sinisa Jakov (1 June 2016). "Macedonia Allows Medical Marijuana in Pharmacies". Balkan Insight. Retrieved 4 November 2017.
- Pace, Maria (27 March 2018). "Malta has officially legalised medical cannabis". Malta Today. Retrieved 24 August 2018.
- Ainge Roy, Eleanor (11 December 2018). "New Zealand passes laws to make medical marijuana widely available". The Guardian. Retrieved 20 January 2019.
- Collyns, Dan (20 October 2017). "Peru legalises medical marijuana in move spurred by mother's home lab". The Guardian. Retrieved 4 November 2017.
- "Medical use of cannabis officially legal in Poland". Radio Poland. PAP. 11 February 2017. Retrieved 4 November 2017.
- Lamers, Matt (21 June 2018). "Portugal passes medical cannabis law, opens domestic market". Marijuana Business Daily. Retrieved 24 August 2018.
- South Asia Regional Profile (PDF), United Nations Office on Drugs and Crime, 15 September 2005, retrieved 2 February 2019
- Mosbergen, Dominique (25 December 2018). "Thailand Approves Medical Marijuana In Regional First". HuffPost. Retrieved 20 January 2019.
- "Medicinal cannabis products to be legalised". BBC. 26 July 2018. Retrieved 28 July 2018.
- "Sativex (delta-9-tetrahydrocannabinol and cannabidiol)". GW Pharmaceuticals. Archived from the original on 10 December 2017. Retrieved 5 November 2017.
- Medical use of cannabis and cannabinoids (PDF), European Monitoring Centre for Drugs and Drug Addiction, December 2018
- Sapra, Bani (20 June 2018). "Canada becomes second nation in the world to legalize marijuana". CNN. Retrieved 3 July 2018.
- Janikian, Michelle (14 September 2017). "Legal Pot In Mexico: Everything You Need to Know". Rolling Stone. Retrieved 5 November 2017.
- Depetris M, Miller J (21 March 2017). "Swiss cannabis entrepreneurs develop craving for low-potency pot". Reuters. Retrieved 5 November 2017.
- Habibi, Roojin; Hoffman, Steven J. (March 2018). "Legalizing Cannabis Violates the UN Drug Control Treaties, But Progressive Countries Like Canada Have Options". Ottawa Law Review. 49 (2).
- "Classification of controlled drugs". European Monitoring Centre for Drugs and Drug Addiction. Retrieved 7 January 2021.
- Kaur, Harmeet (2 December 2020). "The UN removes cannabis from a list of the most dangerous substances". CNN. Retrieved 7 January 2021.
- Kwai, Isabella (2 December 2020). "U.N. Reclassifies Cannabis as a Less Dangerous Drug". The New York Times. Retrieved 7 January 2021.
- "WHO recommends rescheduling of cannabis". European Monitoring Centre for Drugs and Drug Addiction. 25 March 2019. Retrieved 7 January 2021.
- Georgiou, Aristos (8 February 2019). "WHO Recommends Rescheduling Cannabis in International Law for First Time in History". Newsweek. Retrieved 7 January 2021.
- Ingraham, Christopher (13 June 2017). "Jeff Sessions personally asked Congress to let him prosecute medical-marijuana providers". The Washington Post. Retrieved 9 July 2017.
- Timothy B. Wheeler (11 October 2014). "Medical marijuana fees stir debate in Maryland". The Baltimore Sun. Retrieved 12 October 2014.
- Blackwell, Tom (16 October 2013). "The pot vending machine's first foreign market? Canada, of course, 'a seed for the rest of the world'". National Post. Retrieved 4 December 2013.
- "Uber-For-Weed Startup Meadow Lights Up In San Francisco". TechCrunch. AOL. 14 October 2014. Retrieved 22 January 2016.
- "The UK is the world's largest producer of legal Cannabis, UN body finds". The Independent. 7 March 2018. Retrieved 7 December 2020.
- Clark, Tonya Body (10 February 2015). "The Medical Marijuana Debate". Compliance Corner. Wolters Kluwer Financial Services. Retrieved 26 February 2015.
- Peters, Joey (29 June 2015). "Court: Employer can't block workers' comp for medical marijuana". NM Political Report. Retrieved 30 June 2015.
- "Resolution on Medical Marijuana". druglibrary.org. Retrieved 30 July 2017.
- "House of Delegates 2017, Resolution: A8" (PDF). amsa.org. American Medical Student Association. Retrieved 30 July 2017.
- "Medical Marijuana (Cannabis) FAQs". National Multiple Sclerosis Society. Retrieved 30 July 2017.
- Gattone PM, Lammert W (20 February 2014). "Epilepsy Foundation Calls for Increased Medical Marijuana Access and Research" (Press release). Washington, D.C.: Epilepsy Foundation. Retrieved 30 July 2017.
- "Medical Marijuana Use and Research" (PDF). maps.org. Leukemia & Lymphoma Society. Retrieved 30 July 2017.
- "Position Statement on Marijuana as Medicine" (PDF). American Psychiatric Association. Retrieved 30 July 2017.
- Use of Cannabis for Medicinal Purposes (PDF), American Medical Association, 2009
- Supporting Research into the Therapeutic Role of Marijuana (PDF), American College of Physicians, February 2016
- "ASAM Issues New Public Policy Statement on Cannabis" (Press release). Rockville, MD: American Society of Addiction Medicine. 13 October 2020.
- American Heart Association (5 August 2020). "Medical Marijuana, Recreational Cannabis, and Cardiovascular Health". Circulation. 142 (10): e131–e152. doi:10.1161/CIR.0000000000000883. PMID 32752884.
- "Marijuana and Cancer". American Cancer Society. Retrieved 12 July 2017.
- "Marijuana research: Overcoming the barriers". American Psychological Association. 14 September 2017. Retrieved 9 October 2017.
- Arney, Kat (25 July 2012). "Cannabis, cannabinoids and cancer – the evidence so far". Cancer Research UK. Archived from the original on 11 February 2014.
- Reinarman C, Nunberg H, Lanthier F, Heddleston T (2011). "Who are medical marijuana patients? Population characteristics from nine California assessment clinics". Journal of Psychoactive Drugs (Review). 43 (2): 128–35. doi:10.1080/02791072.2011.587700. PMID 21858958. S2CID 23183205.
- "Final Rule: Placement of FDA-Approved Products of Oral Solutions Containing Dronabinol [(-)-delta-9-trans-tetrahydrocannabinol (delta-9-THC)] in Schedule II". U.S. Department of Justice. Retrieved 2 February 2018.
- Clark, Amy (16 May 2006). "'New' Pot Pill For Chemo Patients". CBS News. Associated Press. Retrieved 26 July 2017.
- Abuhasira R, Shbiro L, Landschaft Y (March 2018). "Medical use of cannabis and cannabinoids containing products - Regulations in Europe and North America". European Journal of Internal Medicine. 49: 2–6. doi:10.1016/j.ejim.2018.01.001. PMID 29329891.
- "Produkt – FASS Allmänhet". fass.se.
- Dr Farid F. Youssef. "Cannabis Unmasked: What it is and why it does what it does". UWIToday: June 2010. http://sta.uwi.edu/uwitoday/archive/june_2010/article9.asp
Further reading
- National Academies Of Sciences, Engineering; Health Medicine, Division; Board on Population Health Public Health Practice; Committee on the Health Effects of Marijuana: An Evidence Review Research Agenda (2017). The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. nationalacademies.org. National Academies of Sciences, Engineering, and Medicine: The National Academies Press. doi:10.17226/24625. ISBN 978-0-309-45304-2. PMID 28182367.

External links
| Wikimedia Commons has media related to Medical cannabis. |
- Medical cannabis at Curlie, links to websites about medical cannabis
- Information on Cannabis and Cannabinoids from the U.S. National Cancer Institute
- Information on cannabis (marihuana, marijuana) and the cannabinoids from Health Canada
- The Center for Medicinal Cannabis Research of the University of California
- Medical Marijuana – a 2014–2015 three-part CNN documentary produced by Sanjay Gupta
| General | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Usage |
| ||||||||
| Variants | |||||||||
| Effects | |||||||||
| Culture | |||||||||
| Pro-cannabis organizations | |||||||||
| Use demographics | |||||||||
| Politics |
| ||||||||
| Related | |||||||||
| |||||||||
| |||||||||||||||||||||||||||||||||
